
GIE Associate Editor Shimon Bar-Meir, MD, highlights this article from the May issue: “Utility of repeat colonoscopy attempt after failed colonoscopy: a systematic review and pooled analysis” by Aamir Saeed, MD, et al.

Colonoscopy is the most reliable test for detecting colorectal cancer or colonic polyps. Its advantage lies in being both diagnostic and therapeutic. It allows biopsy specimens to be taken from suspicious lesions and the removal of polyps.
A complete examination of the entire colon, reaching the cecum, should be achieved in at least 95% of cases, and in practice this is even close to 100%. In the current study, the authors identified 26 studies including 1647 patients who had incomplete colonoscopies. In cases where the examination is incomplete, the endoscopist is expected to inform the patient that the procedure was not complete and that it should be repeated—with a colonoscope or alternative equipment such as a pediatric endoscope or balloon-assisted colonoscope.
In such a situation when the first colonoscopy fails, patients who made the effort to prepare for the procedure may feel frustrated, concerned that something went wrong during the procedure, and may lose confidence in their physician. The physician may be embarrassed as well as if he was not technically good enough. He should overcome this feeling and offer a second examination to the patient.
The patient may not understand why a repeat examination would be more successful than the first. It is therefore important to speak with the patient and explain what the issue was and why there is a good chance of at least 95% success on a second attempt (eg, different equipment, a more-experienced examiner, improved bowel preparation, deeper sedation).
It is also important to inform the patient that with a second examination, the likelihood of detecting polyps is about 25%, advanced adenomas approximately 5%, and malignant tumors up to 2%. These numbers are, of course, higher when the examination is performed because of high-risk indications such as a symptomatic patient or a patient with abnormal laboratory test results such as anemia.
This information also is important for the endoscopist, as it highlights the medicolegal risk involved. Understanding that approximately 2% of patients may harbor a malignant tumor emphasizes that, over the course of a professional career, there will likely be cases of cancer that could be missed if a repeat examination is not performed.
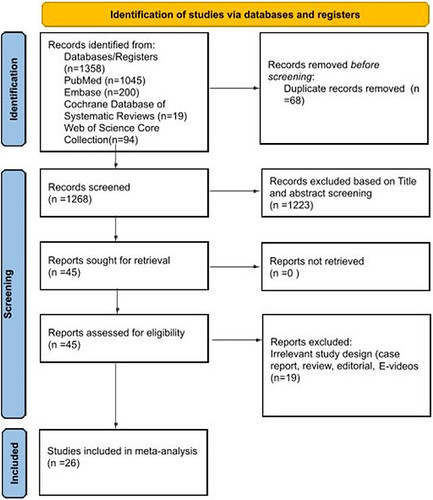
PRISMA flowchart.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
