
 Post written by Zachary L. Smith, DO, from the Division of Gastroenterology, Washington University School of Medicine, St Louis, Missouri, USA.
Post written by Zachary L. Smith, DO, from the Division of Gastroenterology, Washington University School of Medicine, St Louis, Missouri, USA.
The focus of this study was to evaluate the use of general endotracheal anesthesia (GEA) versus monitored anesthesia care (MAC) during ERCP in high-risk patients. Historically, our institution sedated the vast majority of patients via monitored anesthesia care (ie, without an endotracheal tube) for ERCP. Anecdotally, there was suspicion that utilizing GEA for ERCPs would result in a negative impact on the efficiency of the endoscopy unit with an unclear incremental benefit in patient safety. Despite this, there existed no randomized controlled trial to answer this question; therefore, we felt it was important to conduct this study in patients who were at high risk for sedation-related adverse events (SRAE).
A total of 200 patients that met inclusion criteria were randomized to receive either GEA (n=101) or MAC (n=99). The primary endpoint, the composite incidence of SRAE, was higher in the MAC group, and this was primarily the result of a high usage of airway maneuvers for hypoxemia. There were no significant differences in procedure time, cannulation time, fluoroscopy time, or, perhaps most interestingly, in-room time. There was, however, a 10% conversion rate from MAC to GEA for respiratory instability or retained gastric contents. A larger, multicenter randomized controlled-trial would provide more robust evidence, especially with regard to endoscopy unit efficiency.
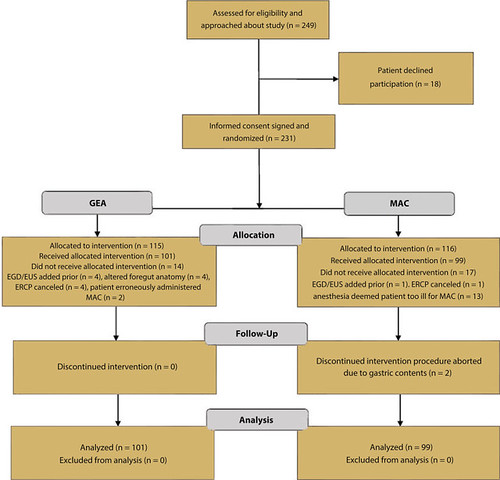
Figure 1. Study flowchart. MAC, Monitored anesthesia care; GEA, general endotracheal anesthesia.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
