
Post written by Asif Khalid, MD, from the Veterans Affairs Pittsburgh HealthCare System, and the University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA. 
Gastroenterologists will don a gown and gloves prior to performing GI endoscopy almost as a reflex, but the use of a face shield is not considered standard practice. This is in spite of most, if not all, of us being able to recall facial splashes occurring during endoscopic procedures. But we still do not use a face shield like we would a gown. We can wash clothes or even dispose of them if they get stained with stool, bile, or blood, but what about our faces and associated mucus membranes? Do years of working in a GI lab make us immune to the feeling of repulsion that the general population would feel if splashed on the face with body secretions? Do we feel the risk of infections such as conjunctivitis, hepatitis C, and HIV is truly negligible because the risk of exposure is negligible? We must wash our hands in between seeing patients, even if we use gloves. Do we wash our faces in between cases, knowing that we touch our faces many times a day without realizing? Since we do not, it must be because the risk of getting splashed in the face during endoscopy is close to if not zero, or is it? We undertook this study to answer this simple question.
It was important to undertake this study, so we could be informed of the risk of exposure to potentially infectious bodily secretions while performing endoscopy. This risk may exist not just for the endoscopist, but also by extension for others we come in contact with including patients, co-workers, and our families. Knowing the incidence of exposure could then lead to individual and organizational efforts to protect endoscopists and others around them.
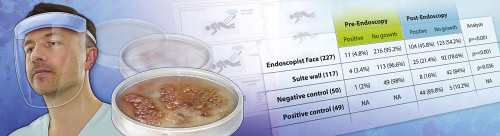
We calculated the number of bacterial colony forming units (CFU) obtained through cultures of face shields prior to endoscopy and after performing a half day of endoscopic procedures. The face shields were placed on the endoscopists faces, on a wall at face level 6 feet away from the patient, and in a location remote from the procedural area. Positive controls included face shields deliberately contaminated with a used scope. We analyzed our data using high thresholds of CFU to detect only definite exposures and not environmental contamination, thus we may have underestimated the true risk of bacterial exposure. Our results suggest that for every 100 half days of endoscopy we perform, we are splashed in the face with bacteria laden patient secretions in over 5 days, and our assistants standing up to 6 feet away are exposed in over 3 of those days. We believe further studies are in order to confirm these results and also identify specific pathogenic organisms.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
