



Post written by Satoshi Kinoshita, MD, Toshio Uraoka, MD, PhD, and Toshihiro Nishizawa, MD, PhD, from the Department of Gastroenterology, National Hospital Organization, Tokyo Medical Center, Tokyo, Japan, and the Department of Gastroenterology and Hepatology, Gunma University Graduate School of Medicine, Maebashi, Japan.
Patients with ulcerative colitis have an increased risk of colorectal dysplasia. Endoscopic submucosal dissection (ESD) for the neoplastic lesions in ulcerative colitis remains controversial. The aim of this study was to clarify the role of ESD in treatment strategy for ulcerative colitis. Consequently, the mean size of resected specimen was 34.9±17.1 mm. The mean procedure time of ESD was 71.3 minutes. En bloc resection and R0 resection rates were achieved in 100% (25/25) and 76% (19/25). During a median 21 months (range 8-80) follow-up, local recurrence did not occur. The biopsy predicted final histological diagnoses of carcinoma with a sensitivity of 72.2% (95% confidence interval [CI], 46.5-90.3), accuracy of 78.2% (95% CI, 56.3-92.5). The endoscopic findings predicted final histological diagnoses of carcinoma with a sensitivity of 72.2% (95% CI, 46.5-90.3), accuracy of 76% (95% CI, 54.9-90.6).
ESD for neoplasms in ulcerative colitis is feasible by expert ESD endoscopists and may avoid an unnecessary surgery. Because biopsy and endoscopic findings had a relatively low accuracy for final histology, ESD could have curative purposes as well as diagnostic purposes. ESD for neoplasms in ulcerative colitis is difficult due to submucosal fibrosis, and should be performed by expert ESD endoscopists with the best suitable equipment and devices.
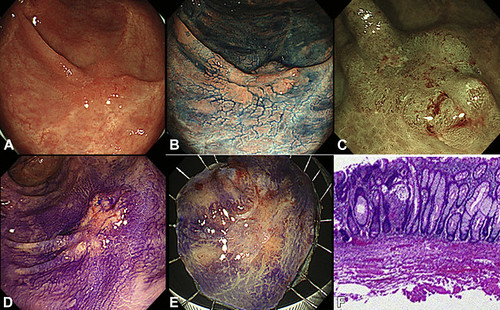
Figure 1. Endoscopic submucosal dissection for adenocarcinoma in a patient with ulcerative colitis. A, A laterally spreading lesion was located in the rectum, 25 mm in diameter. B, Chromoendoscopic view of the lesion stained with indigo carmine. C, Endoscopic view of the lesion with narrow-band imaging. The capillary pattern was IIIA in the Sano classification. D, The pit pattern with crystal violet staining was type VI-low in the Kudo classification. E, Macroscopic view of the resected specimen. Histologic examination of the resected tissue revealed a well-differentiated adenocarcinoma (submucosal invasion 550 μm). Both the vertical and horizontal margins were negative. F, Histologic view of the well-differentiated adenocarcinoma and severe fibrosis in the submucosal layer.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
