
 Post written by Jun Chul Park, MD, from the Division of Gastroenterology, Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
Post written by Jun Chul Park, MD, from the Division of Gastroenterology, Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
Although ESD is performed with curative intent, curative resection of ESD is not always possible. The standard management after noncurative resection (NCR) is additional gastrectomy with lymph node (LN) dissection due to the risk of LN metastasis. However, many recent studies have shown that LN metastasis is found in only 5 to 10% of patients after gastrectomy.
Determining whether or not additional gastrectomy should be performed is a challenge for physicians because many patients tend to be elderly and have many comorbidities. Therefore, patients who were diagnosed with early gastric cancer with NCR tend to undergo additional endoscopic treatment, such as redo-ESD or argon plasma coagulation or even some are left untreated because of old age or poor general condition.
There are still no definite standard treatments for NCR after ESD. There are also not enough data on clinical outcomes after additional endoscopic treatment in relation to the optimal time.
Our study showed that cancer-specific survival and disease-free survival (DFS) were longer in patients who underwent surgery than in those undergoing endoscopic treatment or observation. However, we should consider alternative treatment options for patients with only a positive lateral resection margin after ESD and who cannot undergo additional surgery due to old age, comorbidities, or patient preference. Regarding redo-ESD as an additional endoscopic treatment, redo-ESD is expected to be technically difficult because fibrosis develops within several months. Thus, clarifying the optimal time is important for curative resection.
It is clinically ideal if additional endoscopic treatment is performed early for exact detection of the previous ESD margin (+) site in redo-ESD. However, there is no consistent guideline on the optimal time of additional treatment after NCR ESD for EGC.
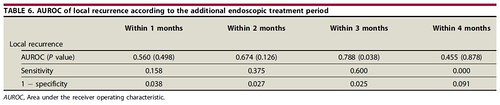
In analyzing our study population, the patients undergoing endoscopic treatment within 3 months showed a lower rate of local recurrence than those undergoing treatment after 3 months, and the intervals on this 3-month basis between primary and additional treatment were shown to be independent predictors.
Therefore, our study could assist the clinician in distinguishing which modality should be used for patients who need additional treatment and when that treatment should be performed, especially regarding redo-ESD in patients with a lower risk of LNM. In addition, we have suggested the optimal time of additional endoscopic treatment in the case of NCR, especially in patients with only a positive lateral resection margin.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
