
 Post written by David S. Zimmon, MD, from the New York University School of Medicine.
Post written by David S. Zimmon, MD, from the New York University School of Medicine.
The author developed multiple biopsy (MB) because forceps biopsy is time consuming, creates endoscopist ergonomic stress, prolongs anesthesia, and adds excessive staff work and workplace risk from soiling, toxic fixatives and sharps. Also MB responds to demands for better patient care, increased productivity, and lower cost.
In a single endoscope pass, MB cuts 25 biopsies of controlled size and depth like a needle biopsy. During endoscope withdrawal, biopsies are collected, oriented, and stored in acquisition order. Biopsies stack like coins in the MB tip. The perforated tip is separated, placed in fixative, and sent to pathology. The endoscopist uses a formatted log that identifies each biopsy by indication, organ, depth, site, and position. Each biopsy pass avoided saves at least 1 minute of procedure and anesthesia time. Shorter procedure time per patent reduces risk and services more patients to increase productivity and income. Faster procedures and dismissal improves patient acceptance. MB improves patient care, reduces manual labor and workplace risk, increases productivity, and reduces cost.
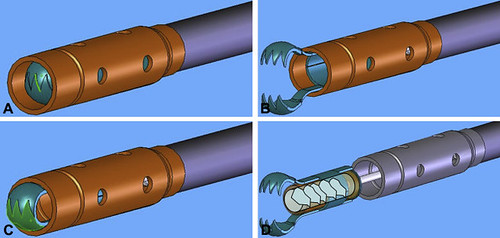
Figure 1. Multiple biopsy function illustrated. A, Jaws retracted into the rounded perforated metal storage cylinder tip for endoscope passage and removal after biopsy sample collection. B, Jaws extended open for tissue insertion to surround biopsy sample. C, Jaws partly closed to surround, cut, and capture a biopsy specimen before retraction into the metal storage cylinder tip. D, Oriented multiple biopsy specimens in the plastic storage chamber inside the biopsy mechanism extended from the metal storage cylinder tip.
Our study established MB safety, efficacy, and clinical value in 67 patients. We then compared colon surveillance biopsies in 15 MB patients to forceps biopsies oriented manually in 15 patients. MB diagnostic value was equivalent to forceps biopsies in this blinded histopathologic study.
Next step: Single-handed MB.
In pathology, the plastic chamber inside the tip, designed for fixation, processing, and microtomy with biopsies in situ, is removed and processed immediately. Plastic chamber processing maintains to the slide, biopsy alignment, orientation, and acquisition order as documented in the endoscopy log. Biopsy loss, damage, and contamination are limited. The work and delay of grossing, processing, and slide production is reduced. Plastic chamber frozen section cancer diagnosis requires 30 minutes or, by microwave processing, 1 to 2 hours. Pathology service is improved by reducing work and workplace risk, speeding diagnosis, increasing productivity, and reducing cost.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Cool! We need il ASAP
Cool! We need it ASAP