
Post written by Jeffrey D. Mosko, MD, MSc, FASGE, FRCPC, from the Division of Gastroenterology, St Michael’s Hospital, Toronto, Ontario, Canada.

This article presents a practical, algorithmic approach to managing incompletely resected colorectal polyps. It covers 8 tips spanning prevention, optimization of standard EMR with margin ablation, adjunctive techniques for fibrotic tissue (hot avulsion, cold avulsion followed by snare tip soft coagulation, snare-tip submucosal release), underwater EMR, hybrid EMR/endoscopic submucosal dissection (ESD), and the selective role of ESD.
As complex resection expands beyond expert centers, more endoscopists are tackling larger and more difficult polyps. As a result, we are seeing more incomplete polyp resections—a major driver of unnecessary surgery and interval colorectal cancer. Yet, despite the many tools and opinions available, there is no consensus on how best to manage these patients.
When invited to contribute to the Top Tips series, I felt it would be useful to share a structured framework that helps endoscopists anticipate complexity, appreciates their limits while safely expanding their toolbox, and aids in keeping patients out of the operating room when endoscopic management is appropriate.
These tips represent my decision framework. Two questions drive technique selection: (1) Does this lesion require en bloc resection for oncologic reasons? (2) Where is the submucosal fibrosis—central, peripheral, or extensive? Central fibrosis usually responds to standard EMR with margin ablation with or without adjuncts; peripheral or extensive fibrosis is where I preferentially use underwater EMR, snare-tip submucosal release, and hybrid EMR/ESD.
Looking ahead, we need better real-world Western data on hybrid and ESD outcomes outside expert centers, clearer patient selection criteria, and structured training pathways so these techniques can travel beyond high-volume sites while maintaining outcomes.
One of the most important messages is tip 8–avoid flailing. One technique will not work for every lesion. Successful resection requires comfort with pivoting midprocedure, and knowing when to refer is as important as knowing how to resect. And with our current resection toolbox, previous partial resection should rarely be considered an indication for surgery.
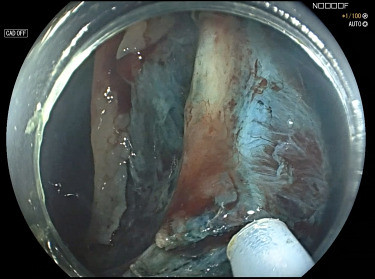
Snare-tip submucosal release of surrounding fibrosis to facilitate complete resection of an area of severe fibrosis.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
