
Post written by Mayank Goyal, MBBS, from the University of Missouri-Kansas City, Kansas City, Missouri, and Mayo Clinic, Rochester, and Manik Aggarwal, MBBS, and Ryan Law, DO, from the Mayo Clinic, Rochester, Minnesota, USA.
This video demonstrates endoscopic management of a complex gastrocolojejunal fistula that developed following EUS-guided gastrojejunostomy (EUS-GJ) in a patient with gastric outlet obstruction secondary to necrotizing pancreatitis.
Severe inflammation likely resulted in inadvertent transcolonic deployment of the lumen-apposing metal stent, creating a multitract communication among the stomach, colon, and jejunum.

The patient presented with septic shock, and initial temporizing therapy included placement of telescoping lumen-apposing metal stents with a coaxial fully covered metal stent to exclude the colon. Definitive therapy was then performed endoscopically using a double-channel gastroscope with OverStitch endoscopic suturing (Boston Scientific, Marlborough, Mass, USA) and over-the-scope clip (OTSC) reinforcement. Both fistulous tracts were successfully closed with fluoroscopic confirmation of complete seal and durable closure on follow-up endoscopy.

As EUS-GJ becomes increasingly used, endoscopists may encounter rare but highly morbid adverse events related to stent misdeployment. To our knowledge, complex gastrocolojejunal fistulas after EUS-GJ are rarely shown in detail, particularly with successful endoscopic rescue and definitive closure.
We felt this case highlighted not only the importance of recognizing these adverse events early but also the expanding role of advanced therapeutic endoscopy as an alternative to high-risk surgery in critically ill patients. The video additionally showcases a multimodal closure strategy combining suturing, OTSC reinforcement, fluoroscopy, and staged endoscopic management.
This case emphasizes several important learning points:
- Severe inflammation can distort anatomical planes during EUS-GJ and increase the risk of transcolonic misdeployment.
- Cross-sectional imaging and fluoroscopy are critical for understanding complex fistula anatomy.
- Advanced endoscopic closure techniques can successfully manage even multitract fistulas in carefully selected patients.
- Combining primary suturing with OTSC reinforcement may improve durability in inflamed or fragile tissue.
- Multidisciplinary planning remains essential when managing these highly complex adverse events.
We hope this video contributes to growing awareness regarding adverse event management after EUS-GJ and features the evolving capabilities of minimally invasive endoscopic therapy for complex GI defects.
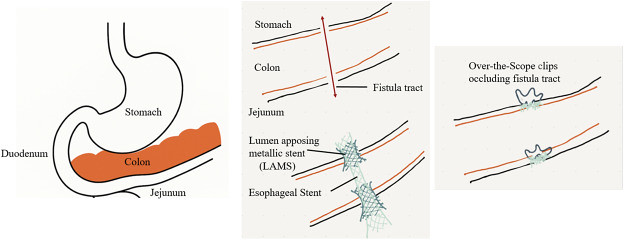
Hand-drawn diagram demonstrating the multitract communication.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
