
Post written by Charing C.N. Chong, MBChB, from the Department of Surgery, and Raymond S.Y. Tang, MD, from the Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong, China.

In this multicenter randomized controlled study, we aimed to compare the diagnostic performance of contrast-enhanced EUS (CE-EUS) and conventional EUS-guided fine-needle biopsy (FNB) with macroscopic on-site evaluation for solid pancreatic lesions.
Timely and accurate tissue diagnosis of solid pancreatic lesions, especially pancreatic cancer, by EUS-guided tissue acquisition can help avoid delay in clinical management. Although prior studies have suggested a lower diagnostic sensitivity of malignancy in pancreatic adenocarcinoma with avascular (necrotic) areas and a potential benefit of CE-EUS in FNA of solid pancreatic lesions, whether the same benefit would be observed when modern dedicated FNB needles with specialized tip design are used remains unclear.

In this international trial comparing diagnostic performance of CE-EUS and conventional EUS-guided FNB with macroscopic on-site evaluation with solid pancreatic lesions, our data show that although the use of contrast could further increase detection of avascular areas from 25.0% to 31.3% in solid pancreatic lesions in the CE-EUS group, the false-negative rates of CE-EUS—guided FNB and conventional EUS-guided FNB were both low without statistical difference (6.0% vs 7.9%, P > .999).
The sensitivity, specificity, and diagnostic accuracy for CE-EUS—guided FNB and conventional EUS-guided FNB were all greater than 90% and comparable. The procedure time was slightly longer in the CE-EUS group (28.9 ± 15.2 minutes vs 24.4 ± 7.7 minutes, P = .039), and the median number of needle passes needed to achieve a macroscopic visible core length ≥4 mm (1 vs 1.5, P = .480) was not statistically different between the 2 groups.
Despite the modest increase in the detection of avascular areas, routine use of CE-EUS did not translate into higher diagnostic yield with solid pancreatic lesions, consistent with recent randomized data from Korea1 and Taiwan2 using FNA/FNB needles. These findings collectively suggest that the superior tissue acquisition capability of dedicated FNB needles may mitigate the negative impact of necrotic areas, reducing the incremental value of CE-EUS for tissue acquisition.
Nevertheless, although routine use of CE-EUS may not be necessary when dedicated FNB needles are used, we believe CE-EUS remains clinically valuable for lesion characterization and detection, especially when lesions are <2 cm.
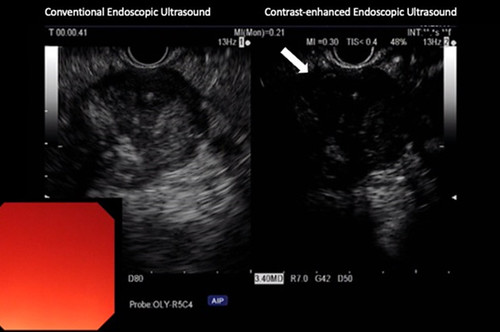
Contrast-enhanced EUS showing a nonenhanced avascular area (white arrow) in a pancreatic mass, suggestive of necrotic area in the lesion.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
- Cho IR, Jeong S-H, Kang H, et al. Comparison of contrast-enhanced versus conventional EUS-guided FNA/fine-needle biopsy in diagnosis of solid pancreatic lesions: a randomized controlled trial. Gastrointest Endosc 2021;94:303-10. ↩︎
- Kuo Y-T, Chu Y-L, Wong W-F, et al. Randomized trial of contrast-enhanced harmonic guidance versus fanning technique for EUS-guided fine-needle biopsy sampling of solid pancreatic lesions. Gastrointest Endosc 2023;97:732-40. ↩︎
