
Post written by Romario Ruiz, MD, and Luis Marin-Calderón, MD, from the Departamento de Aparato Digestivo, Hospital Nacional Edgardo Rebagliati Martins, and Harold Benites-Goñi, MD, from the Departamento de Aparato Digestivo, Hospital Nacional Edgardo Rebagliati Martins, and Vicerrectorado de Investigación, Universidad San Ignacio de Loyola, Lima, Peru.
Our video presents the endoscopic treatment of an 86-year-old man with progressive dysphagia, weight loss, and intermittent oral protrusion of a soft mass. Endoscopy and CT demonstrated a 10-cm pedunculated esophageal fibrovascular polyp arising just distal to the cricopharyngeus without signs of invasion.
Because open surgery would have carried substantial risk in this elderly patient with comorbidities, we performed endoscopic resection with the patient under general anesthesia with orotracheal intubation. Initial endoloop placement with a single endoscope (EG-600ZW; Fujifilm, Tokyo, Japan) was unstable owing to the lesion’s size and mobility.

A second pediatric endoscope (Fujifilm) was therefore introduced alongside the therapeutic endoscope to grasp the distal tip of the endoloop, provide countertraction, and guide the loop securely around the vascular stalk. After mechanical strangulation, hot snare resection and targeted thermocoagulation were completed. The specimen was retrieved intact, and histology confirmed a benign fibrovascular polyp with negative margins. The patient recovered clinically, and no recurrence was noted during 2 years of follow-up.
We felt this video was important because giant esophageal fibrovascular polyps are rare but potentially dangerous lesions. Although benign, they can cause dysphagia, regurgitation, weight loss, airway obstruction, and even fatal asphyxiation. Surgery has traditionally been used for large cervical lesions, but it may be disproportionately morbid in older or high-risk patients. This case demonstrates that an endoscopic approach can be feasible when careful airway protection, preprocedural imaging, and a controlled resection strategy are used. The key educational value of the video is the dual-scope maneuver, which transforms otherwise unstable endoloop placement into a more controlled and reproducible step.
Other endoscopists can learn several practical points. First, preprocedural CT helped confirm the intraluminal, pedunculated nature of the lesion and exclude invasion. Second, superficial biopsy may not be helpful with suspected fibrovascular polyps and can add bleeding risk. Third, placing the endoloop entirely inside the esophagus, without exteriorizing the friable lesion, helped minimize mucosal trauma and airway manipulation. Fourth, the pediatric endoscope acted as a traction and stabilization device, allowing precise endoloop placement at the base of the stalk before transection. Finally, leaving a very small residual base can be reasonable when needed to avoid excessive traction on the esophageal wall; after tight loop placement, ischemic necrosis of the remnant is expected.
We hope this case encourages endoscopists to consider minimally invasive strategies for select patients with giant fibrovascular polyps while recognizing that patient selection, airway protection, multidisciplinary planning, and readiness to manage bleeding or perforation remain essential.
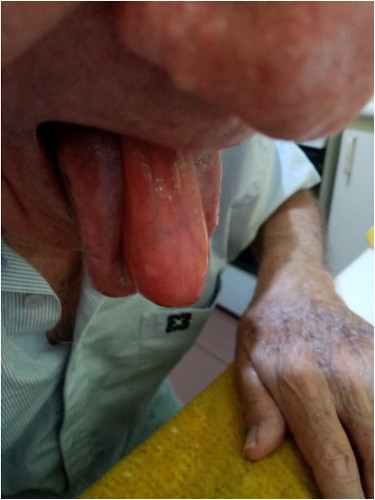
Esophageal fibrovascular tumor protruding through the oral cavity.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
