
Post written by Antonio Facciorusso, MD, PhD, from the Gastroenterology Unit, Department of Surgical and Medical Sciences, University of Foggia, Foggia, Italy.

In the last decade, several EUS fine-needle biopsy (FNB) sampling needles have been developed, and newer end-cutting FNB needles, which feature alterations of the cutting tip, have been found to outperform other needles in terms of diagnostic yield for tissue sampling of pancreatic masses.
Moreover, several tissue sampling techniques—such as slow pull, dry suction, modified wet suction, and no suction—have been tested.
Evidence on the comparative diagnostic yield of these sampling techniques is limited. Meta-analyses including studies with FNA have provided conflicting results, and no definitive assumptions on this topic are recommended in the current guidelines.
In the last few years, several randomized controlled trials (RCTs) compared EUS-guided tissue sampling techniques in patients with pancreatic masses, and hence there is a pressing need to systematically analyze the growing body of evidence in the field to inform clinical practice.
In contrast with pairwise meta-analyses, network meta-analyses can inform comparative effectiveness of multiple interventions and synthesize evidence across a network of RCTs. Using this approach, we made several key observations. Modified wet suction ranked as the best performing technique to obtain higher rates of adequate samples, whereas the no-suction technique was significantly inferior to the other interventions.
Furthermore, modified wet suction significantly outperformed dry suction in terms of tissue integrity and ranked as the best intervention regarding this parameter.
Slow-pull and dry-suction techniques showed similar adequacy results, although with significantly less blood contamination in the case of slow pull. Modified wet suction seemed to be associated with higher rates of samples with blood contamination; however, this had little clinical impact on the diagnostic outcomes.
Rapid on-site cytologic evaluation (ROSE) was generally unavailable in the included RCTs, and definitive assumptions on the comparative efficacy of different sampling techniques in the presence of ROSE could not be drawn.
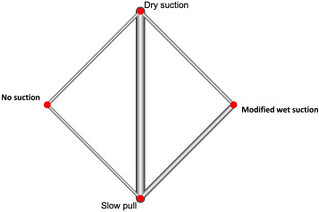
Network of included studies with available direct comparisons between different strategies for EUS-guided FNA of pancreatic masses. The size of the nodes and thickness of the edges are weighted according to the number of studies evaluating each intervention and direct comparison, respectively.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
