
Post written by Yoko Kubosawa, MD, from the Division of Gastroenterology and Hepatology, Department of Internal Medicine, and the Division of Research and Development for Minimally Invasive Treatment, Cancer Center, Keio University School of Medicine, Tokyo, Japan.
We analyzed the incidence of post–endoscopic submucosal dissection (ESD) strictures after wide-field duodenal ESD.
Although it is known that lesions occupying a large circumference are associated with the risk of post-ESD strictures in other organs, the corresponding data for duodenal lesions are unknown.
A total of 80 lesions were included, and 2 involved mucosal defects occupying more than 90% of the circumference. None of the lesions caused delayed perforation and stricture. Only 6 lesions resulted in luminal narrowing, which occurred more frequently in lesions with mucosal defects occupying a larger circumference.
The mucosal defect was closed, at least partially, in 90% of all lesions and in 86% of lesions with mucosal defect occupying more than 75% of the circumference. When we examined by the degree of closure, luminal narrowing occurred about 3 times more frequently in the incomplete closure group (15%) than in the complete closure group (5%).
In particular, for lesions with mucosal defects occupying more than 75% of the circumference, the incidence of luminal narrowing was 0% in the complete and incomplete closure groups but 100% in the nonclosure group.
When ulcers heal, they shrink from the edges in all directions toward the center. Contraction in the short-axis direction more frequently leads to strictures because of the limited room in the lumen.
With the string clip suturing method we use, both the anal and oral edges of the mucosal defect are hauled in by the string and sutured. Thus, the mucosal defect shrinks in the long axis and deforms only slightly in the short axis.
The Kerckring’s fold in the duodenum consists of only the mucosa and submucosa and does not contain a proper muscle layer, and there is a surplus of mucosa to the muscle layer. Therefore, even when a large mucosal defect is hauled in and sutured, strong closure is maintained. Suturing may prevent post-ESD stricture formation.
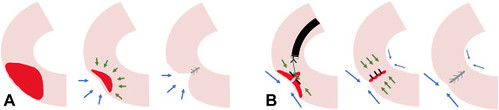 Schemas of the healing process of mucosal defects. A, The healing process when the mucosal defect was not closed. B, The healing process when the mucosal defect was closed with the string clip suturing method.
Schemas of the healing process of mucosal defects. A, The healing process when the mucosal defect was not closed. B, The healing process when the mucosal defect was closed with the string clip suturing method.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
