
Post written by Madhav Desai, MD, MPH, from the Division of Gastroenterology, Hepatology, and Nutrition, University of Minnesota Medical Center, Minneapolis, Minnesota, USA.

Achieving an optimal adenoma detection rate (ADR), a priority quality metric for screening colonoscopy, is necessary for a high-quality colonoscopy. Studies have shown that a higher ADR is linked to a lower risk of interval colon cancers.
A withdrawal time of 6 minutes is considered a minimum threshold for a standard colonoscopy and has been established as a quality metric. However, the threshold beyond which ADR does not increase further is unknown.
A colonoscopy withdrawal time of at least 6 minutes has been recommended to maximize ADR, but this is prone to gaming. Multiple studies have shown that ADR is higher with a longer withdrawal time (6 to 9 minutes vs 6 minutes), but robust data from a randomized controlled trial setting are lacking on how long the withdrawal time should be to capture the maximum benefit. Data on sessile serrated lesion detection rate and withdrawal time also are unavailable.
We examined withdrawal time (excluding polyp resection/bowel cleaning time) of subjects undergoing screening and/or surveillance colonoscopy in a prospective, multicenter, randomized controlled trial (NCT03952611). We explored the impact of withdrawal time in 1-minute increments on ADR and reported odds ratios (ORs) with 95% confidence intervals (CIs).
Overall, 1142 subjects (mean age, 62.3 ± 8.9 years; 80.5% men) underwent screening (45.9%) or surveillance (53.6%) colonoscopy. We found that ADR continued to rise significantly for a withdrawal time of 6 minutes to ≥11 minutes (50.4% vs 65.1%), suggesting a higher yield with a higher withdrawal time.
There was an upward trend in ADR probability until a withdrawal time of approximately 13 minutes, beyond which ADR did not increase further (Figure). Withdrawal time was noted to significantly increase in parallel with the adenoma-per-colonoscopy metric as well.
For the sessile serrated lesion detection rate, maximum impact was noted by a withdrawal time of 10 minutes, and then there was a downtrend. For every 1-minute increase in inspection time, there was a 6% increased likelihood of a higher ADR (OR, 1.06; 95% CI, 1.02-1.10; P = .004).
However, this effect was not demonstrated for the sessile serrated lesion detection rate metric (OR, .92; 95% CI, .84-1.01; P = .064).
Results from this multicenter, randomized controlled trial show an incremental increase in ADR (6% with every additional minute) with a withdrawal time up to 13 minutes. There was no further increase in adenoma detection beyond that time.
Therefore, we recommend aiming for a quality withdrawal time of at least 6 minutes and up to 13 minutes during a screening and surveillance colonoscopy among average-risk patients to achieve optimal ADR and a high-quality exam. This means spending adequate time to clean and examine behind folds and performing a thorough meticulous inspection in the colon on withdrawal rather than a time target only.
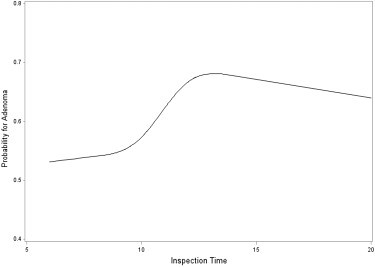 Spline graph examining the impact of an increase in withdrawal time on probability of ADR.
Spline graph examining the impact of an increase in withdrawal time on probability of ADR.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
