
Post written by Partha Pal, MD, DNB, MRCP (UK), from the Department of Medical Gastroenterology, Asian Institute of Gastroenterology, Hyderabad, India.

In this study, we compared single-balloon enteroscopy with motorized spiral enteroscopy in suspected Crohn’s disease (CD) in a prospective manner. We aimed to compare the technical success, diagnostic yield, depth of maximal insertion, enteroscopy time, and adverse events between both procedures.
When we systematically reviewed the literature prior to initiation of the study, we found certain knowledge gaps. No study had ever prospectively compared balloon-assisted enteroscopy with motorized spiral enteroscopy in suspected CD.
Moreover, we realized that diagnostic yield in suspected CD depends not only on the ability to reach the lesion for technical success, but it also takes into account the ability to make a diagnosis based on endoscopic impression and histology.
This is why this should be evaluated separately from suspected vascular lesions, which may require a total enteroscopy more often. We found that most of the studies on the role of suspected CD are silent on histological yield, and no prospective data address what happens when a patient is treated based on endoscopic impression without histological confirmation.
More importantly, it was unclear from the literature which modality of enteroscopy can be used for suspected CD, given both available modalities. Hence, we conducted the study.
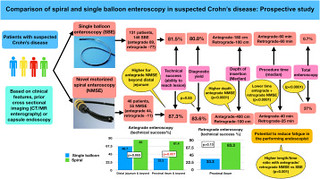
In total, 177 patients with suspected CD (37.2% female; aged 7-75 years) underwent a total of 201 enteroscopy procedures. Motorized spiral enteroscopy had higher technical success for deeper intestinal lesions, significantly higher depth of insertion in a shorter time (higher length-to-time ratio [cm/min]), and complete small-bowel coverage rate (37% vs .7%). This could have important implications for performing enteroscopy more efficiently, saving time and reducing fatigue for the performing endoscopist.
The overall technical success (the ability to reach the lesion) with single-balloon enteroscopy (81.5%) was similar to that of motorized spiral enteroscopy (87.3%), except for deeper small-bowel lesions (proximal ileal and beyond) in which the technical success of motorized spiral enteroscopy (81.4% vs 33.3% for the antegrade route) was higher and can be a preferable option.
The overall diagnostic yields were not different. Histology was confirmatory for CD in 20.4% and suggestive in 61.1%. The rest were treated successfully with medications, with a follow-up of 6-15 months. Both modalities were safe with minimal adverse events.
However, balloon enteroscopy can be preferred in high-risk patients unfit for general anesthesia and pediatric and postoperative patients. Hence, the choice between both modalities in suspected CD should be based on prior cross-sectional imaging, availability, experience with both modalities, and the clinical characteristic of the patient with suspected CD.
As for the future, a randomized, parallel study design with consecutive procedures is needed to confirm these findings.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
