
Post written by Wiriyaporn Ridtitid, MD, and Rungsun Rerknimitr, MD, from the Division of Gastroenterology, Department of Medicine, Faculty of Medicine, Chulalongkorn University, and the Excellence Center for Gastrointestinal Endoscopy, King Chulalongkorn Memorial Hospital, Bangkok, Thailand.

The focus of this randomized trial was to compare bacterial contamination evaluated by culture between duodenoscopes with disposable distal caps and duodenoscopes with fixed distal caps after manual cleaning.
Currently, the standard of duodenoscope reprocessing consists of 5 steps: precleaning, leak testing, manual cleaning, high-level disinfection (HLD), and drying and storage.
However, several outbreaks of multidrug-resistant bacterial contamination have been reported in duodenoscopes with fixed distal caps after standard reprocessing because of the complex elevator mechanism.

Based on previous studies, there was no significant benefit of supplement methods of duodenoscope cleaning such as double HLD, ethylene oxide gas sterilization, and liquid chemical sterilization after standard reprocessing.
In addition, the U.S. Food and Drug Administration (FDA) has recommended surveillance or per-procedure microbiological culturing and quarantine to ensure no bacterial contamination after reprocessing. Because use of culture is not feasible in real practice with every procedure with the 72-hour waiting period for culture results, the adenosine triphosphate (ATP) test has been widely accepted as a reliable audit tool for duodenoscope cleaning.
Our previous data proposed an ATP threshold of 40 relative light units (RLUs) to ensure effectiveness of HLD, given its sensitivity of 100% with a negative predictive value of 100% for bacterial contamination.
Although the FDA has recommended newly designed duodenoscopes with disposable components to improve cleaning the elevator back site, data on the contamination rate of duodenoscopes with disposable distal caps after manual cleaning and HLD are still lacking.
In our study, we found that, after manual cleaning, duodenoscopes with fixed distal caps had a significantly higher proportion of bacterial contamination than duodenoscopes with disposable distal caps (14% vs 7%, P = .02).
After manual cleaning, the mean ATP level also was significantly higher in duodenoscopes with fixed distal caps than duodenoscopes with disposable distal caps. After initial HLD, the proportion of potential bacterial contamination (using the ATP threshold of ≥40 RLUs after HLD) in duodenoscopes with fixed distal caps was 2.7 times higher than duodenoscopes with disposable distal caps but did not reach statistical significance (4% vs 1.5%, P = .13).
The conclusion of this study is that duodenoscopes with disposable distal caps provide a significantly lower rate of bacterial contamination and organic residue after manual cleaning than duodenoscopes with fixed distal caps because of the ability to access the back side of the elevator for more meticulous cleaning. Only a few duodenoscopes from each group did not pass the ATP threshold after HLD.
We did not include other designs of duodenoscopes such as duodenoscopes with detachable caps and elevators. Therefore, additional studies are warranted to test other designs of duodenoscopes.
Further cost analyses among strategies to minimize the risk of duodenoscope-related infection (including standard HLD, double HLD, ethylene oxide gas sterilization, culture and quarantine, duodenoscopes with disposable distal caps, and single-use duodenoscopes) are required to confirm these outcomes.
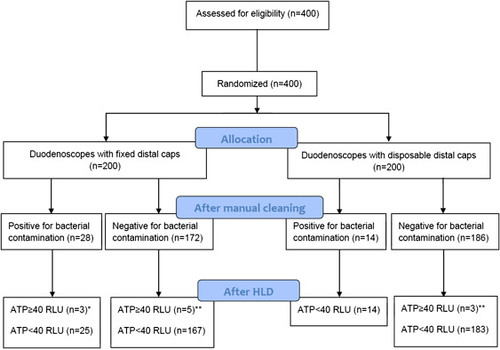 Flowchart of the study. ∗One and 2 duodenoscopes required 3 and 2 high-level disinfection (HLD) cycles, respectively, to pass the adenosine triphosphate (ATP) threshold. ∗∗All duodenoscopes required 2 HLD cycles to pass the ATP threshold. RLU, Relative light unit.
Flowchart of the study. ∗One and 2 duodenoscopes required 3 and 2 high-level disinfection (HLD) cycles, respectively, to pass the adenosine triphosphate (ATP) threshold. ∗∗All duodenoscopes required 2 HLD cycles to pass the ATP threshold. RLU, Relative light unit.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
