
Post written by Hiroyuki Aihara, MD, PhD, from the Division of Gastroenterology Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, USA.

A 40-year-old woman with persistent upper abdominal pain was found to have a 3-cm subepithelial lesion in the prepyloric area and was referred to our center.
EUS showed an anechoic cyst in the submucosa with well-defined outer sonographic borders suggesting a gastric duplication cyst (GDC). The cyst was aspirated and yielded 40 mL of serous fluid with negative cytology for malignancy.
The patient’s symptoms resolved for 3 weeks but then recurred. A CT scan showed a cystic lesion with diameters of 3.2 × 1.2 × 1.1 cm. Therefore, the decision was made to remove the cyst with endoscopic submucosal dissection (ESD).
During ESD, we encountered a 2-mm vessel-like structure that appeared to originate from the cyst and enter the muscularis propria. After achieving complete skeletonization of the duct, 2 hemoclips were deployed at its distal and proximal sides, and the duct was then cut through between the clips using an ESD knife. The duplication cyst was completely dissected in an en bloc fashion.
The connection of GDC to pancreatic ducts is a rare but well-documented phenomenon, with 25 reported cases in the literature. This connection could be to a bifurcated pancreatic duct, or more commonly, to the duct of an accessory pancreatic lobe, and recurrent pancreatitis can be seen in 60% of these cases.
Unroofing is an alternative strategy, but there is a concern for reaccumulating cystic fluid owing to the remaining cystic wall and a communicating duct underneath the gastric mucosa. In most cases, surgical resection is recommended. However, ESD has emerged as an alternative, minimally invasive approach with the recent developments in endoscopic surgery.
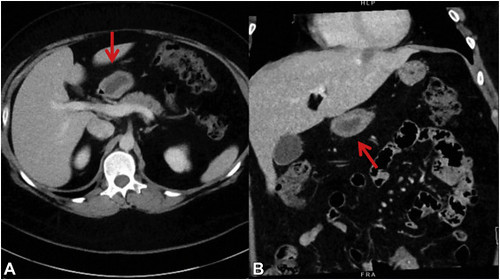 Sagittal (A) and coronal (B) sections of the abdominal CT scan with contrast demonstrating the cystic lesion (arrows) with diameters of 3.2 × 1.2 × 1.1 cm in close proximity to the pancreatic body but without any pancreatic abnormalities.
Sagittal (A) and coronal (B) sections of the abdominal CT scan with contrast demonstrating the cystic lesion (arrows) with diameters of 3.2 × 1.2 × 1.1 cm in close proximity to the pancreatic body but without any pancreatic abnormalities.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
