
Post written by Gursimran Kochhar, MD, from the Mayo Clinic, Jacksonville, Florida.
Fistulas indicate one advanced disease phenotype in patients with IBD. Currently, there is no definitive therapy for management of fistulas. Medical therapy is not adequate, and surgical therapy forms the cornerstone of management of fistulas in patients with IBD. Although surgical therapy is effective, it is invasive and can have significant complications. We wanted to focus on use of endoscopic techniques in the management of fistulas in carefully selected patients so as to avoid surgery if possible. The idea of this study was to show a new technique to our readers, which can be used in a selected group of patients with IBD in addition to standard medical and surgical therapy techniques.
A total of 29 patients were included in the study who underwent endoscopic fistulotomy. The mean age of patients undergoing the procedure was 44.2 ± 14.6 years. Twenty-six patients had IPAA, and 3 patients had an ileocolonic resection. The most common location of fistula in our cohort was the pouch body (48.2%). A total of 13 patients (44.8%) had a concurrent stricture and were treated with endoscopic stricturotomy. Nine of these patients had endoscopic stricturotomy prior to fistulotomy, while 4 had simultaneous endoscopic therapy for stricture and fistula.
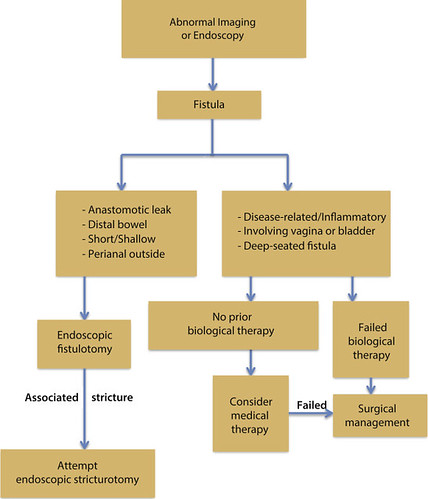
Figure 4. Algorithm depicting management of a fistula in inflammatory bowel disease.
All 29 patients had initial technical success in endoscopic fistulotomy, 19 (34.4%) only needed 1 endoscopic session. The mean number of endoscopic sessions for the successful healing of the fistula was 1.9 ± 0.7. Endoscopic fistulotomy was clinically successful in 26 patients (89.6%), while 3 (10.4%) eventually required surgery to manage their fistulas. No perforations were observed in our cohort. One patient (3.4%), however, developed significant bleeding.
The doctrine of endoscopic therapy for fistula is adopted from that in surgical literature. Among endoscopic treatment modalities, fistulotomy, if feasible, is preferred to closure with clipping or fistula track injection. In our i-IBD Unit, endoscopic fistulotomy has become the first-line therapy and a standard of care for carefully selected patients.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
