
Post written by Giovanni D. De Palma, MD, from Department of Clinical Medicine and Surgery, University Federico II of Naples, School of Medicine, Naples, Italy.
Our paper presents a single-center, randomized, back-to-back trial which was designed to investigate the contribution of the EndoCuff device to the improvement of the adenoma eetection rate in the course of standard colonoscopies.
Before this study, EndoCuff had been investigated only in the context of randomized parallel trials, which indeed showed positive results, with improvements of the adenoma detection rate up to 14.7 percentage points. However, parallel trials suffer from some important limitations when they compare the diagnostic proficiency of 2endoscopic techniques. Indeed the observed difference in the adenoma detection rate among the 2 groups might reflect also a real difference in the prevalence of adenomas, which might persist despite randomization. So, the 2 techniques are better tested on the same patients, by back-to-back studies.
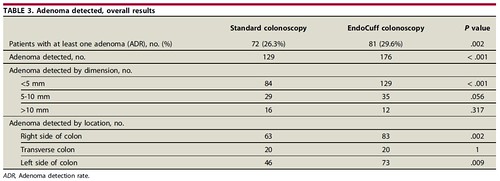
274 patients participated to the study. Each patient underwent same-day tandem colonoscopies with and without EndoCuff, in an order decided in a random manner. The 2 procedures followed each other and were performed by the same endoscopist in the same endoscopic suite. Olympus high-definition colonoscopies were used for all procedures. Polyps found in the course of the first procedure were left in situ and were removed at the end of the second procedure. Only lesions proven to be adenomatous at histology were considered in the analysis and classified according to size and location. A total of 285 polypoid lesions were excised and 188 were found to be adenomatous at histology. The statistical analysis showed that EndoCuff improved the Adenoma detection rate by 3.28% compared to standard colonoscopy. The total number of detected adenomas also increased by 36%, determining an increase of the mean number of detected adenomas per patient, which is a further indicator of the quality of colonoscopy. Additional adenomas detected by EndoCuff were mainly small (<5 mm) and located in the right and left colon. In addition, EndoCuff determined a more correct interval of surveillance in about 6% of patients, following the current US guidelines. In our study, Endocuff improved the diagnostic proficiency of colonoscopies by increasing the identification of diminutive adenomas, which indeed rarely have high-risk features and progress very slowly into cancer. Whether this really contributes to the prevention of interval carcinomas remains debatable. However, 2 aspects have to be kept in mind. The Adenoma detection rate is mainly determined by small adenomas, which are the majority of adenomas and, nevertheless, a predictor of interval cancer. In addition, identification of multiple diminutive adenomas helps in defining the risk of the patient developing advanced adenomas and CRC and, consequently, the correct interval of surveillance. Our study has several strong points due to its design but also some limitations, which are discussed in the paper. The main limitation is that the study involved patients undergoing endoscopy for several reasons: diagnostic, screening, or surveillance. This makes findings applicable to daily practice. However, the prevalence of adenomas is different among these categories of patients and, consequently, the diagnostic profit of EndoCuff might be different according to the indication. This topic needs to be addressed by tailored studies together with dedicated economic analysis, which need to quantify the cost-benefit ratio, primarily in comparison with other new techniques (eg, full spectrum endoscopy).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
