
 Post written by Takemasa Hayashi, MD, from the Digestive Disease Center, Showa University Northern Yokohama Hospital, Yokohama, Japan.
Post written by Takemasa Hayashi, MD, from the Digestive Disease Center, Showa University Northern Yokohama Hospital, Yokohama, Japan.
This study focuses on the incidence of stenosis and its relationship with the clinicopathological factors in surveillance. Endoscopic submucosal dissection for large colorectal neoplasms can reduce the need for unnecessary surgery. Large mucosal lesions should be removed endoscopically. I felt it was necessary to clarify the risk of stenosis after ESD for large lesions.
Circumferential mucosal defect of more than 90% is a significant risk factor for stenosis after colorectal ESD. Surveillance endoscopy 6 months after ESD is recommended to assess for development of stenosis. Defects smaller than 90% do not require close endoscopic follow-up or prophylactic measures for prevention of post-ESD stenosis. After endoscopic submucosal dissection for large colorectal neoplasms, stenosis risk is very low compared to other digestive organs. Early surveillance after endoscopic treatment will increase detection of stenosis. The sufficient interval between treatment and surveillance provide the time for narrow lumen to dilate naturally with bowel movement and feces. 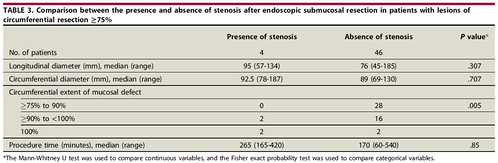 Find the article abstract here.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
