
 Post written by Jun Chul Park from the Division of Gastroenterology, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine.
Post written by Jun Chul Park from the Division of Gastroenterology, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine.
In deciding on a treatment method for EGC that is considered to be within the expanded criteria, both patients and doctors may feel burdened by the probability of additional surgery after ESD because additional gastrectomy after ESD can lead to waste of medical resources and expense and increase the risk for adverse events. Therefore, to avoid unnecessary procedures, clinicians usually strive to select suitable patients with EGC who meet the criteria before procedure. However, until now, there has been no accurate model that can predict non-curative resection of ESD in patients with EGC. This kind of predictive model can be very useful to both doctors and patients in the clinical field. Therefore, we constructed this study to reduce the rate of unnecessary operations with non-curative resection by using variable endoscopic findings.
Various risk factors associated with non-curative resections of ESD in EGC or lymph node metastasis have been published in recent studies. However, studies focused on various endoscopic gross findings, including atrophy, exudates, or fold shape, are very rare. We wanted to find useful clinical risk factors and establish a predictive model that can be used before deciding whether to perform ESD.
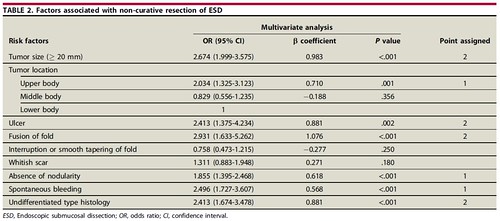
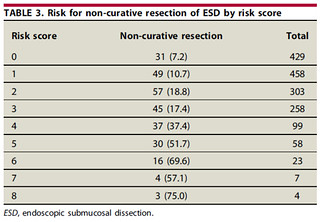
Comparing non-curative ESD and curative ESD groups, we found that 7 factors were significantly different between the 2 groups in the multivariate analysis. The 7 factors were large tumor size, tumor location in the upper body, ulcer, fusion of gastric folds, absence of mucosal nodularity, spontaneous bleeding, and undifferentiated tumor histology. Points of risk scores were assigned to these variables, and the risk scores ranged from 0 to 8. As the total risk score increased, the risk for non-curative resection of ESD increased from 7% to 75%. Our prediction scoring model showed good discriminatory performance among the 2000 bootstrap internal samples.
This scoring method can be used easily in the clinic. Clinicians can pay close attention to patients who are classified in the high-risk group, and this can lead to reductions in unnecessary procedures and medical expense. In addition, we can easily explain to the patient about the possibility of additional surgery after ESD.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
