
 Post written by Shashideep Singhal from the University of Texas Health Science Center at Houston.
Post written by Shashideep Singhal from the University of Texas Health Science Center at Houston.
A 63-year-old man with a long-standing history of achalasia presented for pneumatic dilation. Several technical problems were associated with pneumatic balloo dilation in this case, which had resulted in failure of an earlier attempt. Because of a tortuous megaesophagus with sharp, nearly 90-degree angulations, there was significant looping of the gastroscope in the esophagus and difficulty advancing the pneumatic balloon catheter over the guidewire. Furthermore, the patient had copious amounts of retained food because of the development of the megaesophagus. A 50cm-long gastric overtube with an outer diameter of 19.5mm was introduced into the stomach, and the position of the gastroesophageal junction (GEJ) was marked externally on fluoroscopy with the use of a metal paper clip. After guidewire advancement into the stomach, the pneumatic balloon catheter was introduced through the overtube, which allowed for a straighter passage into the stomach. The overtube was then withdrawn proximally to the balloon, and pneumatic dilation was performed.
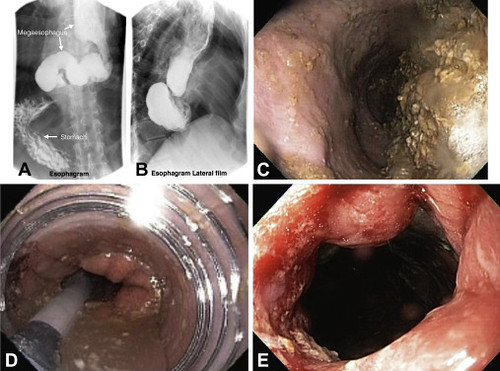
Figure 1. A, Frontal projection of barium esophgram showing megaesophagus/sigmoid esophagus. B, Lateral projection of barium esophagram. C, Dilated esophagus with food. D, Achalasia pneumatic balloon catheter inside overtube. E, Gastroesophageal junction post dilation.
Dilation of achalasia is an effective treatment in select patients, especially those who are not surgical candidates. Tortuous esophagus can sometimes limit ability to effectively perform achalasia dilation leading to significant morbidity in these patients. This technique can improve the technical success and reduce procedure time in achalasia with tortuous esophagus.
The use of a long overtube allows relatively straight passage of a balloon catheter even through a tortuous esophagus, and it allows maintenance of the position at the GEJ for pneumatic dilation in previously failed cases. This technique requires no special devices and can be done in most endoscopy centers with standard equipment.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
