
Post written by Louis M. Wong Kee Song from the Mayo Clinic.
 The aim of the study was to evaluate the efficacy and safety of over-the-scope clip-assisted endoscopic full-thickness resection (EFTR) technique for removal of epithelial and subepithelial lesions in the GI tract.
The aim of the study was to evaluate the efficacy and safety of over-the-scope clip-assisted endoscopic full-thickness resection (EFTR) technique for removal of epithelial and subepithelial lesions in the GI tract.
EFTR allows for definitive diagnosis and treatment of select subepithelial and epithelial GI lesions that are not amenable to conventional resection techniques, such as endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD). Although various techniques to achieve EFTR have been described, the over-the-scope clip-assisted EFTR is technically less demanding and involves: (1) thermal marking of the periphery of the lesion; (2) lesion suction into the cap of the over-the-scope clip device, with or without triprong anchor retraction of the lesion; (3) clip deployment; and (4) en bloc resection of the lesion above the clip using an electrosurgical snare and/or knife. Data regarding the efficacy and safety of this technique, however, are scant.
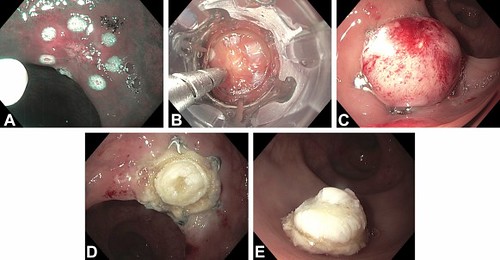
Figure 4. A, Narrow-band imaging of small, biopsy specimen–proven, scarred, neuroendocrine tumor marked with argon plasma coagulation. B, Padlock clip with triprong anchor retraction device. C, Lesion pseudo-polyp above the deployed Padlock clip. D, Resection defect. E, En bloc resected specimen.
We reported on nine patients who underwent the procedure for subepithelial lesions in the duodenum (n=4), rectosigmoid colon (n=2), and stomach (n=1), as well as postappendectomy appendiceal orifice polyps (n=2). The mean lesion size was 8±3 mm, and the mean procedure time was 53±21 minutes. R0 resection (negative margins) was confirmed in all cases. The histopathological diagnoses included neuroendocrine tumors (n=6), sessile serrated adenomas (n=2), and pancreatic heterotopia (n=1). No adverse events were noted. In our series, commercially available over-the-scope clip devices and resection accessories were used for EFTR of lesions throughout the GI tract. The size of the resected specimen is determined, in part, by the size of the over-the-scope cap selected. The use of the over-the-scope clip-assisted EFTR technique, therefore, is limited to resection of lesions that are less than 1 to 2 cm in size. Larger sample size studies are awaited to confirm the efficacy and safety of over-the-scope clip-assisted EFTR.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
