
Post written by Rohit Sinha, MBBS, MRCP, PgDip, from the Royal Infirmary and The University of Edinburgh, Edinburgh, United Kingdom.
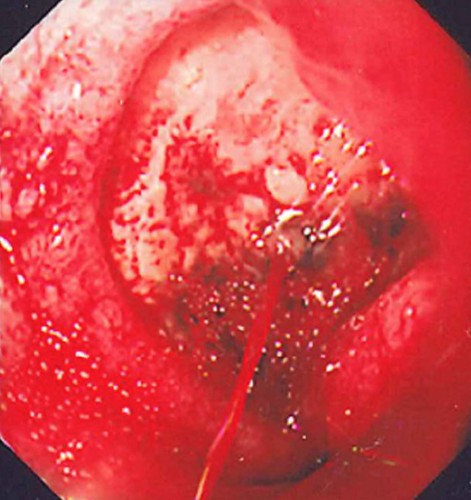
We wanted to evaluate the efficacy of Hemospray in conjunction with established hemostatic endo-therapy in a high-risk nonvariceal upper GI bleeding setting. There was no evidence about the efficacy and outcome of combination therapy (Hemospray plus adrenaline alone or adrenaline with either hemostatic clip and/or heater probe).
The “unknown” composition of Hemospray unsettles endoscopists. In addition, it seems counter-intuitive that spraying powder would stop a lethal bleed. Consequently, this skepticism is reflected in the real-world practice of endotherapy. It is interesting to observe that in our small cohort of high-risk peptic ulcer bleeds and when compared to pre-hemospray era, the outcomes are better, and it does complement the conventional therapy. Perhaps it is not a bad idea after all, to use it as a belt-and-brace approach to maximize the hemostatic goal, although the “proprietary” nature of powder leaves me ambivalent. Would I reach out for hemospray next time I am struggling to satisfy myself with conventional endo-therapy? I think I will.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
