
Kenichiro Imai from the Division of Endoscopy, Shizuoka Cancer Center presents this video case.
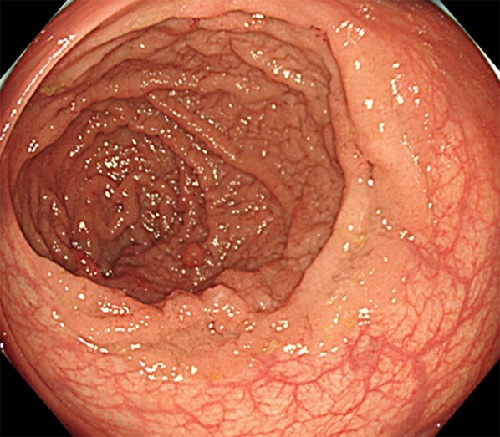
We demonstrated complete circumferential colorectal endoscopic submucosal dissection (ESD) using an insulated-tip knife. Colonoscopy in a 70-year-old woman showed a 15-cm circumferential laterally spreading tumor (LST) in the upper rectum. Through the use of magnified endoscopy, we diagnosed non-invasive cancer, so we decided to perform ESD. To achieve en bloc resection, we applied the submucosal tunneling technique. Submucosal tunneling was safely done by a “push-and laterally dissect” technique using an insulated knife (ITknife nano™, Olympus, Tokyo). After submucosal tunnel creation, submucosal dissection of the surrounding submucosal tissue was performed. By the use of conscious sedation (Midazoram and Pethidine), the patient could change her position, conveniently. The full use of the gravity force from the patient’s position changes effectively maintained good traction effects. Complete en bloc resection was achieved without any adverse events. Histology was intramucosal adenocarcinoma with negative lateral and vertical margins. Prophylactic steroid anal administration (2mg/day) was started a week after ESD; however, an obstructive symptom occurred 3 weeks after ESD, and stenosis was confirmed endoscopically. A more severe stenotic change at the oral side of the ulcer indicated that steroid suppository did not reach the whole of the ulcer. We changed to performing repeated balloon dilation combined with local injection of triamcinolone (100mg/2wks). Mucosal heeling was confirmed 3 months after ESD, and she had no symptoms.
Recently, endoscopic resection has been recommended as an initial therapy not only for adenoma/ carcinoma in situ but for T1 cancer. For lesions suspicious of cancer, histological evaluation is crucial for tumor staging. Higher incidence of submucosal invasion is expected in large lesions, so precise histological evaluation is increasingly demanding. However, endoscopic resection for extremely large colorectal lesions is considered technically challenging. Moreover, the management of possible stenosis is problematic. This case shows technical feasibility of complete circumferential ESD and success of stenosis management, which suggests expanding the boundaries of endoscopic resection for circumferential LSTs.
Submucosal tunneling endoscopic resection has been reported in the esophageal region, such as in POEM procedures. The colorectal wall has more complex shapes owing to the semilunar folds than the esophagus, thus, a submucosal tunneling procedure in the colorectal region has an increased risk of perforation. Because more tunnel creations may lead to an increased risk of perforation, only one submucosal tunneling is optimal. Moreover, submucosal dissection around the tunnel using patient’s position changes is easy and time-saving. Our strategy with the combination of a single submucosal tunneling and submucosal dissection with patient’s position changes may make the best use of an insulated-tip knife and may be a potentially feasible method for complete circumferential ESD.
Find more VideoGIE cases online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
