
 Alejandro L. Suarez, MD, from the Division of Gastroenterology & Hepatology at the Medical University of South Carolina in Charleston, South Carolina, USA writes about this video case “Stepwise endoscopic resection of a large gastric lipoma causing gastric outlet obstruction and GI bleeding.”
Alejandro L. Suarez, MD, from the Division of Gastroenterology & Hepatology at the Medical University of South Carolina in Charleston, South Carolina, USA writes about this video case “Stepwise endoscopic resection of a large gastric lipoma causing gastric outlet obstruction and GI bleeding.”
Lipomas of the gastrointestinal tract are slow growing tumors commonly found incidentally. Although rare, symptomatic lipomas are traditionally managed surgically. With the advent of modern endoscopy, these lesions can be managed less invasively, obviating the need for surgery. In this case video we demonstrate the endoscopic management of a large gastric lipoma causing gastric outlet obstruction and GI bleeding.
A 54-year-old woman with coronary artery disease on Aspirin and Plavix presented to the hospital complaining of melena and gastric outlet obstructive symptoms for several days. She had normal hemodynamics in the setting of acute blood loss anemia. After cessation of Plavix she underwent an upper endoscopy. Using a standard gastroscope a large lipoma measuring approximately 4 cm in size was visualized in the gastric antrum with its distal end prolapsing through the pyloric channel. Due to its large size and concern for excessive electrocoagulation potentially leading to gastric wall muscle injury, the decision was made to resect the lesion in a stepwise fashion.
Using a standard endoscopic mucosal resection (EMR) technique, half of the lesion was resected. Although, a large amount of fat capsule was exposed, enucleation of the lesion was unsuccessful. There were no procedure-related complications. Repeat endoscopy was performed due to persistent symptoms, revealing a residual lipoma still partially obstructing the pyloric channel. It was removed with a standard polypectomy snare, resulting in near-complete removal of the lipoma, and resolution of symptoms. Repeat endoscopy three months later revealed healed mucosa overlying the resected site and visualization of a non-obstructed pyloric channel.
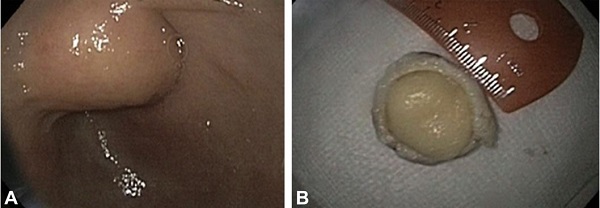
Figure 1. A, Gastric lipoma obstructing the pylorus. B, Endoscopically transected gastric lipoma specimen.
Different endoscopic platforms exist to remove gastrointestinal lesions, each with merits and disadvantages. For example, en-bloc resection can be achieved with endoscopic submucosal dissection (ESD), but requires a prolonged procedure time and carries a higher risk profile than standard EMR, even in expert hands. On the other hand, although our case required a repeat procedure, it was performed utilizing standard EMR techniques that do not require advanced training or experience. Stepwise resection may have decreased the risk of muscle injury by avoiding prolonged electrocoagulation immediately adjacent to the gastric wall, particularly in the high fat containing lesions such as lipoma, which are poor conductors of electricity.
Find more VideoGIE cases online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
