
 Navin L. Kumar, MD, and John R. Saltzman, MD, FASGE from the Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, in Boston, Massachusetts, USA discuss this Review article, “Initial management and timing of endoscopy in nonvariceal upper GI bleeding.”
Navin L. Kumar, MD, and John R. Saltzman, MD, FASGE from the Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, in Boston, Massachusetts, USA discuss this Review article, “Initial management and timing of endoscopy in nonvariceal upper GI bleeding.”
The focus of our article was to review the existing literature on the initial management of acute nonvariceal upper GI bleeding (UGIB), including fluid resuscitation, blood transfusion, management of anti-thrombotics, and risk stratification. We also devote a full section to timing of upper endoscopy in these patients.
UGIB from a nonvariceal source is a frequent cause of hospital admission and commonly encountered by physicians of all specialties. In order to provide the best care for these patients, it is of utmost importance to use evidence-based medicine to guide management. In this article, we provide the evidence both in favor and against certain treatment strategies in UGIB. We hope our work will allow clinicians to make informed decisions when dealing with this common presentation. 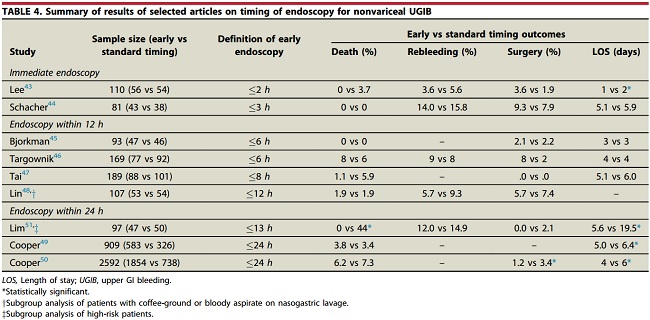
Advances in medical and endoscopic therapy have led to significant declines in the in-hospital mortality rate for nonvariceal UGIB. The initial steps of management include fluid resuscitation with isotonic intravenous fluids, a restrictive transfusion strategy to transfuse for hemoglobin levels <7 g/dL (except if exsanguinating bleeding or significant cardiovascular comorbidities), and withholding of anti-thrombotics. Proton-pump inhibitor therapy should be started promptly upon presentation, and patients should undergo risk stratification based on existing validated scores such as the Glasgow-Blatchford Score (GBS) or AIMS65 score.
After the patient is adequately resuscitated, the next step in management is upper endoscopy, which should be performed within 24 hours of presentation. However, patients with very low-risk of adverse outcomes (e.g. Glasgow-Blatchford Score of 0) may be managed safely as outpatients. Urgent endoscopy (within 12 hours of presentation) is associated with an increased use of endoscopic therapy without an improvement in clinical outcomes. However, there may be a benefit of urgent endoscopy for select patients at higher-risk of bleeding, and future studies involving the use of prognostic scores to inform the optimal timing of endoscopy are needed. Patients with upper GI bleeding initially managed based on best available current evidence will have optimal outcomes.
Read the full article through the GIE website.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
