
 Zhao-Shen Li, MD, from the Department of Gastroenterology, Changhai Hospital, The Second Military Medical University, in Shanghai, China discusses this Original Article, “Extracorporeal shock wave lithotripsy is a safe and effective treatment for pancreatic stones coexisting with pancreatic pseudocysts.”
Zhao-Shen Li, MD, from the Department of Gastroenterology, Changhai Hospital, The Second Military Medical University, in Shanghai, China discusses this Original Article, “Extracorporeal shock wave lithotripsy is a safe and effective treatment for pancreatic stones coexisting with pancreatic pseudocysts.”
The focus of this study was the application of pancreatic extracorporeal shock wave lithotripsy (P-ESWL) in chronic pancreatitis (CP) patients with both large pancreatic stones and pancreatic pseudocyst (PPC).
The coexistence of PPCs and large stones (≥5 mm) in CP cases is not rare. In fact, 7% (59/849) of the cases in the current study accounts for this condition. However, no such instance was mentioned in the any guidelines and consensus. ERCP alone often fails to extract the stones and clear the obstruction. A multistep strategy, which includes EUS-guided PPC drainage and followed ESWL plus ERCP to clear stones. renders high cumulative risk and low success rate. Surgery is sometimes performed as a complementary method or a primary choice, although it is highly invasive. In the current study, we posed a simplified micro-invasive strategy, initial P-ESWL combining ERCP, and its safety and efficiency have been confirmed. 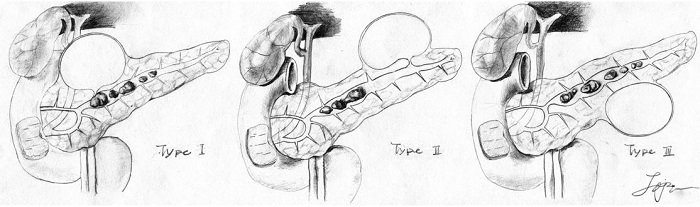
Figure 2. Three types of PPC secondary to calcified CP. Type I, PPC is directly associated to large stones: a communicating PPC is located near the stones that obstruct the MPD and communication passage thereby directly causing PPC formation. Type II, PPC indirectly associated to large stones: a communicating PPC is at a considerable distance from the stones that obstruct the MPD, thereby indirectly causing PPC formation. Type III, PPC is seemingly not associated to large stones: a noncommunicating PPC coexists with MPD obstructed by stones (some tiny communicating passages that are undetectable by ERCP may exist). (Illustrated by J.-J.T.) PPC, pancreatic pseudocyst; CP, chronic pancreatitis; MPD, main pancreatic duct.
P-ESWL combined with post-ESWL ERCP is a safe and effective strategy for stone clearance and PPC regression for patients with both large pancreatic stone and PPC. With this treatment, complete and partial stone clearance was 87.93% and P-ESWL complication rate did not increased compared to that in CP without PPC. PPCs disappeared in 76.36% (42/55) of the patients after 1 year and pain improvement was achieved in 89.09% of the patients. A randomized control study is expected to reconfirm the advantages of the initial P-ESWL strategy against multistep-intervention strategy and surgery in patients with coexisting calcified CP and PPCs.
We proposed a classification scheme for PPCs in CP cases on the basis of the spatial relationship among the pancreatic duct, stones, and PPCs (Figure 1). Types I and II PPCs, which are supposedly communicating with the pancreatic duct, mostly disappeared during the follow-up period. More than half of the Type III PPCs disappeared during the follow-up period possibly because PPCs are drained through tiny communicating passages and decreased pressure in MPD facilitates PPC drainage. Overall, PPCs disappeared in 76% of the patients. But, the efficiency of the initial P-ESWL combined with ERCP strategy on PPC regression was evaluated using the auto-control design, and PPCs may achieve spontaneous resolution without any interventions. Thus, the efficiency of this strategy on PPC regression needs further confirmation.
Read the full Open Access article here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
