
 Rajesh Krishnamoorthi, MD, from the Division of Gastroenterology and Hepatology, Department of Internal Medicine, at Mayo Clinic in Rochester, Minnesota, USA discusses this systematic review and meta-analysis “Risk of recurrence of Barrett’s esophagus after successful endoscopic therapy.”
Rajesh Krishnamoorthi, MD, from the Division of Gastroenterology and Hepatology, Department of Internal Medicine, at Mayo Clinic in Rochester, Minnesota, USA discusses this systematic review and meta-analysis “Risk of recurrence of Barrett’s esophagus after successful endoscopic therapy.”
Endoscopic therapy is currently the treatment of choice for Barrett’s esophagus (BE) related dysplasia and mucosal adenocarcinoma. While the success rate with endoscopic therapy is promising, previous estimates of recurrence of intestinal metaplasia (IM) after achieving complete remission of CRIM has widely varied. We performed a systematic review and meta-analysis to reliably estimate an accurate recurrence risk after CRIM. 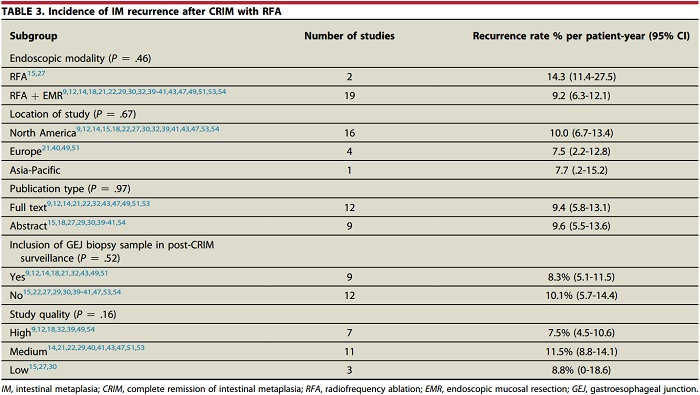
We felt it to be important for several reasons. Firstly, the recurrent disease after CRIM could be dysplastic Barrett’s esophagus or carcinoma, which may require further endoscopic therapy or esophagectomy. Secondly, there are no guidelines on duration of follow-up and frequency of surveillance endoscopies after achieving CRIM. Thirdly, the cost-effectiveness of endoscopic therapy depends on durability of CRIM and need for additional therapy of recurrent disease.
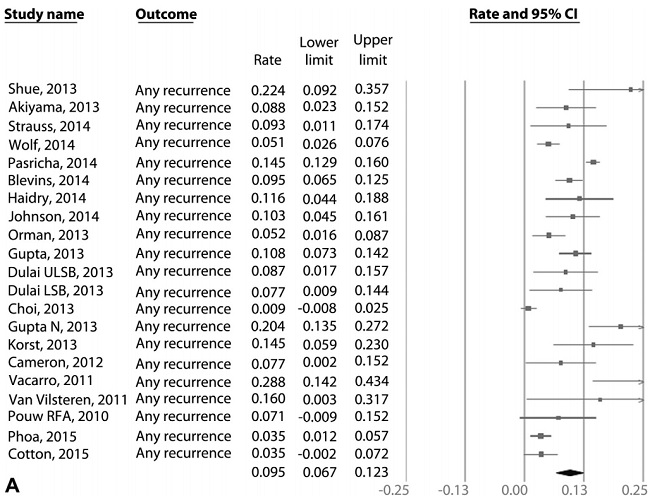 Figure 3. A, Incidence of recurrent IM after achieving CRIM using RFA in patients with BE.
Figure 3. A, Incidence of recurrent IM after achieving CRIM using RFA in patients with BE.
Based on meta-analysis of 21 radiofrequency ablation (RFA) studies, pooled incidence rate of recurrent intestinal metaplasia, dysplastic BE, and high-grade dysplasia (HGD)/ esophageal adenocarcinoma (EAC) after achieving CRIM were 9.5%, 2.0%, and 1.2% per patient-year, respectively. The incidence of recurrence after achieving CRIM was substantial. A small minority of recurrences were dysplastic BE and HGD/EAC. Hence, continued surveillance after CRIM is imperative. Additional studies with long-term follow-up are needed.
Increasing age and Barrett’s segment length were predictive of recurrence. 97% of the recurrences were treated endoscopically, which highlights the importance of surveillance after CRIM. Substantial heterogeneity was noted in the meta-analysis.
Find the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
