
 Sauid Ishaq, FRCP, from the Department of Gastroenterology, Russells Hall Hospital, Birmingham City University in Birmingham, United Kingdom discusses this systematic review and meta-analysis: “Flexible endoscopic treatment for Zenker’s diverticulum: a systematic review and meta-analysis.”
Sauid Ishaq, FRCP, from the Department of Gastroenterology, Russells Hall Hospital, Birmingham City University in Birmingham, United Kingdom discusses this systematic review and meta-analysis: “Flexible endoscopic treatment for Zenker’s diverticulum: a systematic review and meta-analysis.”
The aim of this systematic review was to pool the results of endoscopic treatment of Zenker’s diverticulum (ZD) in terms of efficacy and safety, as well as to address relevant clinical, pathophysiologic, and technical issues where this information was available. Division of septum using flexible endoscope using cutting devices is a new and emerging technique first described by Chris Mulder 1995 along with others. Since then variations of the technique have been reported using different devices. All these studies were in the form of small case series- with variable outcome in success and recurrence. A group of experts felt the need of a systemic review to make some sense of what has been published in the past. The aim was to pool results of endoscopic treatment for ZD in terms of success, adverse events, and recurrence. 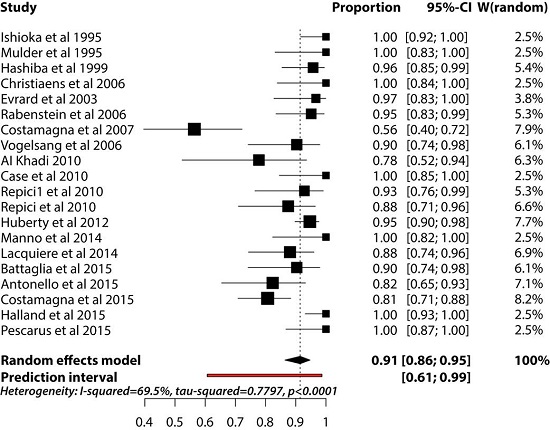
Figure 2. Results of random effects meta-analysis of the proportion of successes. The squares represent individual studies, and the size of the square represents the weight given to each study in the meta-analysis. Error bars represent 95% confidence intervals. The diamond represents the combined results. List of studies shows the name of the first author and the year of publication
According to this meta-analysis, flexible endoscopic septum division (FESD) treatment for ZD is effective and safe. Our results showed that this treatment option is associated with a pooled success estimate of 91%, a pooled adverse event rate estimate of 11.3%, and a pooled recurrence rate estimate of 11%.
Our systematic review indicated a high degree of heterogeneity among studies. This appeared to be mainly related to the small sample size of the selected studies. Randomized controlled trials of flexible endoscopy versus open surgery may be unethical, but large, prospective, multicenter studies are needed to validate further endoscopic advances. There is also the need for improved standardization in terms of symptom evaluation and objective scoring, as well as clear definitions of success, relapse, and adverse events.
Read the abstract for this article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Congratulations for the valued publication and insightful research.