
GIE Associate Editor Alessandro Repici, MD, recommends this article from the May issue: “Incremental diagnostic yield of chromoendoscopy and outcomes in inflammatory bowel disease patients with a history of colorectal dysplasia on white-light endoscopy” by Parakkal Deepak, MBBS, Gregory J. Hanson, MD, Joel G. Fletcher, MD, et al.
The role of careful examination with CE of patients with dysplasia detected with WLE. Additional CE is extremely useful in increasing the diagnostic yield especially disclosing new lesion which have not been identified with standard WLE. Moreover is important the message that patients with long-standing UC and diagnosis of visible or invisible dysplasia should be referred to tertiary level center with expertise in IBD patients and chromoendoscopy. Additional chromoendoscopy is very valuable also to define lesions resectability which allowed to spare surgical resection in most of the patients included in this retrospective analysis.
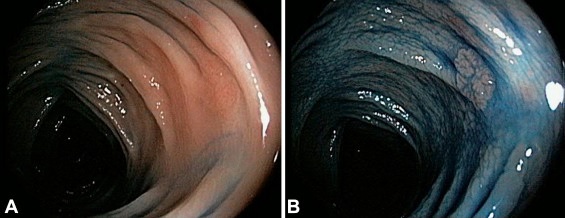
Figure 1.White-light endoscopy (A) and chromoendoscopy (B) demonstrating a flat lesion with low-grade dysplasia.
This is a study showing what is the real scenario in clinical practice of management of patients with IBD and dysplasia. The role of chromoendoscopy as well as therapeutic management of lesions (most of whom located in the right colon) are nicely described in the paper. CE increases the diagnostic yield also in patients with dysplasia identified with WLE. In accordance with SCENIC consensus, CE should be always performed in long-standing UC patients both improving diagnosis of dysplasia and characterize lesions resectability. Referral of difficult dysplastic patients to center with expertise in the field is mandatory.
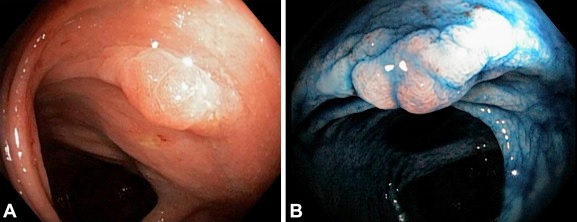 Figure 2. White-light endoscopy (A) and chromoendoscopy (B) demonstrating a large, sprawling 3-cm sigmoid polyp.
Figure 2. White-light endoscopy (A) and chromoendoscopy (B) demonstrating a large, sprawling 3-cm sigmoid polyp.
Read the article abstract here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
