
 David L. Diehl, MD, FACP, FASGE, from the Department of Gastroenterology and Nutrition, Geisinger Medical Center, in Danville, Pennsylvania, USA discusses this article, “EUS-guided liver biopsy provides diagnostic samples comparable with those via the percutaneous or transjugular route.”
David L. Diehl, MD, FACP, FASGE, from the Department of Gastroenterology and Nutrition, Geisinger Medical Center, in Danville, Pennsylvania, USA discusses this article, “EUS-guided liver biopsy provides diagnostic samples comparable with those via the percutaneous or transjugular route.”
Endoscopic ultrasound guided liver biopsy (EUSA-LB) is an emerging technique for performing liver biopsy. In patients who already need an endoscopic procedure, a liver biopsy can be done during the same sedation with little added time. We have previously shown that EUS-LB gives adequate amounts of tissue for pathological diagnosis, but unique to other methods of liver biopsy, can sample widely separated regions of the liver.
To establish the role of EUS-LB among the available techniques of liver biopsy, it is important to demonstrate that tissue yields are at least equivalent to those obtained by the percutaneous or transjugular routes. This study was designed to make that quantitative comparison in terms of portal count, total specimen length, and length of the longest piece of liver tissue.
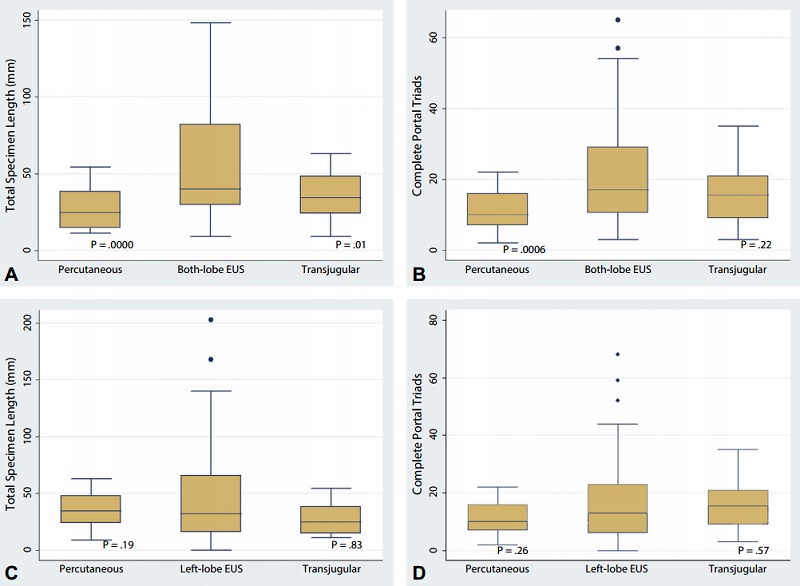
Only non-cirrhotic cases were included to avoid biasing the study against the transjugular route which is most commonly done in cirrhotic livers. This study demonstrated that EUS-LB produces usable pieces of liver tissue at least equivalent to those obtained by the percutaneous or transjugular routes. EUS-LB allows “bilobar” biopsy which results in more tissue obtained, and can also serve to control for regional differences in distribution of hepatic pathology. Performing EUS-LB along with an EGD or EUS when there are concomitant indications for both can make the combination cost-effective, and this is likely to be the source of the most growth of the EUS-LB procedure in the future.
Future directions for study include working out the optimal technical methods for the EUS-LB procedure, including needle type and gauge, amount of suction, number of passes, and specimen handling.
Read the abstract for this article here.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
