
 Shashideep Singhal, MD, form the Division of Gastroenterology, Hepatology and Nutrition, University of Texas Health Science Center, in Houston, Texas, USA presents this video case, “Endoscopic closure of iatrogenic duodenal perforation using dual over-the-scope clips.”
Shashideep Singhal, MD, form the Division of Gastroenterology, Hepatology and Nutrition, University of Texas Health Science Center, in Houston, Texas, USA presents this video case, “Endoscopic closure of iatrogenic duodenal perforation using dual over-the-scope clips.”
A 44-year-old female was referred for endoscopic retrograde cholangiography (ERC) after an intraoperative cholangiogram done during laparoscopic cholecystectomy for acute cholecystitis revealed common bile duct stones. A duodenoscope was advanced to the duodenum without difficulty. A 1.5 cm full thickness perforation was found in the anterior wall of the second portion of the duodenum immediately after duodenoscope insertion. The ERC was aborted. The duodenal perforation was closed using two over-the-scope clips (OTSCs 12/6 gc). CT scan of the abdomen with oral gastrograffin contrast was performed after endoscopic perforation closure and showed free intraperitoneal and retroperitoeal air, however no leakage of enteric contrast was seen. An upper GI series with gastrograffin was done at Day 9 and showed no contrast leak. Two OTSCs were seen in the KUB. A follow up MRI/MRCP was performed at Day 45, which showed resolution of air fluid collection, no leak of oral contrast and resolution of biliary filling defects likely due to spontaneous passage of stones.
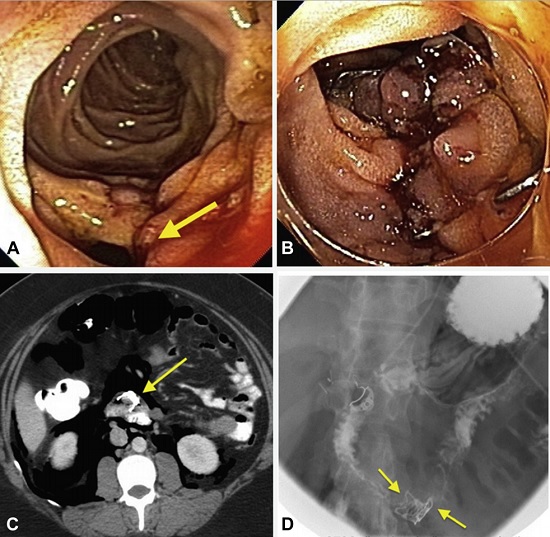
Figure 1. A, Duodenal perforation. B, Over-the-scope clip (OTSC) closure of perforation. C, CT image showing pneumoperitoneum and OTSC clip. D, Upper GI series without leakage of contrast medium (day 10). Arrows show OTSCs placed adjacent to each other.
Perforation of the duodenum is a rare adverse event of upper gastrointestinal endoscopy, which is traditionally managed surgically and is associated with significant morbidity and mortality. This video demonstrates the technique of using OTSCs for successful closure of duodenal perforation.
The technique of using two OTSCs can be helpful in select cases where the defect is larger or at a location where closure with a single OTSC might be difficult. In this case, a twin grasper was passed through the channel of the endoscope to oppose the edges of the duodenal wall defect and pull it into the OTSC cap. The first OTSC was applied to the site of the defect. A small residual defect was visible after placement of first OTSC. A second OTSC was placed adjacent to the first clip at the site of residual defect using suction technique. Satisfactory closure of defect was achieved.
OTSCs are important additions to the endoscopic armamentarium of general gastroenterologists as well as therapeutic endoscopists for successful closure of gastrointestinal perforations and avoid surgery.
Find more VideoGIE cases online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.

Congratulations for the excellent presentation. I wonder when it would be considered safe to repeat ERCP in this situation.
It will ideally be better to wait for 4-6 weeks to perform ERCP to help the damaged tissue gain enough strength. If there are clinical parameters that warrant an urgent ERCP such as cholangitis, I will go for it earlier.
Thank you for your prompt and precise reply, Dr. Singhal.