
Post written by Michael Lajin, MD, from Sharp HealthCare, San Diego, California, USA.

We present a case series of 3 patients with helical stenosis after surgical sleeve gastrectomy treated with modified gastric peroral endoscopic myotomy (G-POEM) as the initial approach. All patients in this series underwent under-saline tunneling, which facilitated navigation through a swirling, challenging submucosal (SM) space. This article offers techniques and tips for successfully completing the procedure.
Helical stenosis is an adverse event of surgical sleeve gastrectomy, characterized by axial rotation of the gastric tube at the incisura angularis, resulting in functional obstruction and increased intragastric pressures. This can lead to early disruption of the staple line below the gastroesophageal junction after surgery, leading to serious adverse events such as leaks or gastric fistulas. Other symptoms include regurgitation, refractory acid reflux, and inability to tolerate food.
This condition is often underdiagnosed. Patients frequently present with years of refractory reflux symptoms and nonhealing esophagitis despite not having a significant hiatal hernia and being treated with proton pump inhibitors. This may contribute to the high prevalence of Barrett’s esophagus (11%) among the sleeve gastrectomy group.1
Severe regurgitation can even mimic achalasia. Patients may see multiple gastroenterologists and undergo numerous endoscopies and imaging tests without discovering the underlying cause of their symptoms. Some may even undergo antireflux surgery with no relief.
During endoscopy, a clockwise rotation of the staple line is observed, resulting in varying degrees of luminal narrowing. The gastroscope usually passes through the twisted section with a torquing maneuver without significant difficulty. This may explain why this functional obstruction is often overlooked.
Although stenting and dilation may help with nonhelical stenosis, these techniques do not cause sufficient muscle tearing. A modified G-POEM technique was recently introduced to treat gastric sleeve stenosis by performing SM tunneling followed by myotomy at the twisted part of the stomach, promoting remodeling of the stricture.
Limited data are available on modified G-POEM for treating gastric sleeve stenosis, but, to our knowledge, our case series is unique in that it focuses specifically on patients with helical stenosis and uses modified G-POEM as the primary endoscopic treatment.
Our SM tunnel was made on the posterior wall of the greater curvature, facilitating easier tunnel entry and avoiding the surgical staple line. The challenge of creating a SM tunnel that swirls along a helical twist within a wispy, fibrotic SM layer was addressed using these tips:
- Use saline immersion therapeutic endoscopy to continuously expand the SM space and protect the mucosa.
- Maintain the dissection plane immediately above the muscularis propria.
- Regularly exit the tunnel to evaluate its direction.
- Keep the SM tunnel wide to facilitate assessment of its overall course.
- Help maintain excellent visibility through meticulous preventative coagulation of blood vessels.
All patients underwent a full-thickness myotomy. The myotomy was initiated distally and progressed proximally stepwise for the following reason: the gastroscope shaft exerts some pressure against the gastric wall as it passes through the helical stenosis.
In other words, the gastric wall in the proximal part of the twist helps support advancement of the scope toward the distal part. Starting full-thickness myotomy proximally might hinder scope advancement and make it difficult to complete the myotomy distally.
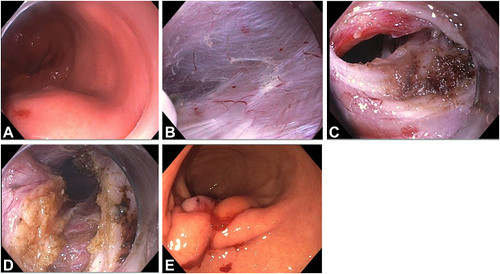
Patient 1. A, Submucosal injection proximal to the stenosis. B, Submucosal dissection under saline solution. C, Endoscopic view of the gastric angulation inside the tunnel after completing the submucosal tunneling. D, A 7-cm full-thickness myotomy was completed. E, The tunnel entry was closed with OverStitch suturing (Boston Scientific, Marlborough, Mass, USA).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
- Qumseya BJ, Qumsiyeh Y, Ponniah SA, et al. Barrett’s esophagus after sleeve gastrectomy: a systematic review and meta-analysis. Gastrointest Endosc 2021;93:343-52.e2. ↩︎
