
Post written by Giuseppe Vanella, MD, PhD, from IRCCS San Raffaele Scientific Institute and Vita-Salute San Raffaele University, Milan, Italy, Michiel Bronswijk, MD, from University Hospitals Gasthuisberg, University of Leuven, Leuven, and Imelda General Hospital, Bonheiden, Belgium, and Roy L.J. van Wanrooij, MD, PhD, from Amsterdam UMC, Vrije University, Amsterdam, The Netherlands.

EUS-guided gastroenterostomy (EUS-GE) is one of the major breakthroughs in modern endoscopy. For patients with gastric outlet obstruction, it offers a minimally invasive way to restore enteral intake while avoiding some of the limitations of enteral stenting and surgical bypass.
At the same time, anyone who has performed or observed this procedure or has heard about it at conferences knows that EUS-GE is not a single universally standardized technique. Different centers have developed different habits: how to distend the jejunum, where to target the loop, how to deploy the lumen-apposing metal stent (LAMS), how to confirm correct placement, and how to react when things do not go as planned.
Our study was designed to bring these different experiences into the same room and ask a practical question: what do experienced operators actually agree on? The motivation to conduct this study came from daily clinical practice. EUS-GE is powerful, but it is also technically demanding. When a procedure is complex and heterogeneously performed across centers, the learning curve is steep, and uncertainty can slow adoption and may affect outcomes.
We had spent years refining our own approaches and exchanging experiences with colleagues worldwide. At some point, it felt like the right moment to sit down together, not to debate which technique is “better,” but to map out what most experienced operators actually agree on.
What was needed was a structured attempt to distinguish the core principles of the procedure from the areas where practice is still evolving. The modified Delphi process allowed us to do this in a transparent way, with anonymous voting, repeated feedback, and international input from experts who have helped shape the technique.
The most reassuring finding was that, despite differences in technique, there was broad agreement on several key safety principles. Experts strongly supported the need of fluoroscopy, careful management of aspiration risk, use of assisted technique (with a catheter in the jejunum) and saline for jejunal distention, preference for freehand deployment of electrocautery-enhanced LAMS placement, and the need for operators to be proficient in managing adverse events such as bleedings and perforations. The stronger-than-expected agreement on preferring a 20-mm LAMS also stood out: despite limited high-quality comparative data, experienced operators have developed a shared clinical intuition that the broader anastomosis pays off.
Equally important, however, were the areas where consensus was less complete. The best target loop, the role of contrast or dye, and whether to routinely dilate the stent all generated discussion. The discussion around misdeployments was some of the richest in the whole process. It surfaced a real tension between extreme endoscopic salvage rather than involvement of the surgeon, with the final statements trying to reflect that nuance. We see this not as a weakness, but as one of its strengths: these unresolved points define the agenda for future research, training, and device development.
For us, this project was less about declaring 1 technique superior and more about making EUS-GE safer, more teachable, and more reproducible. We hope these recommendations will help experienced endoscopists refine their practice, support centers beginning an EUS-GE program, and stimulate prospective studies addressing the questions that remain open.
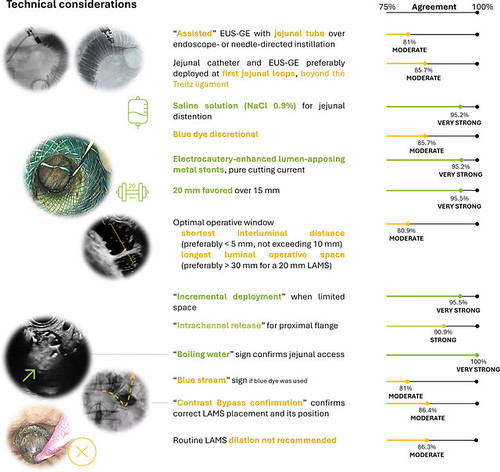
Graphical summary of statements regarding EUS-GE technical considerations: bar length is proportional to the percentage of consensus, shown on a scale from 50% to 100% at the bottom of the figure. Expert agreement is also summarized through colors: dark green (very strong agreement); green (strong agreement); yellow (moderate agreement). EUS-GE, EUS-guided gastroenterostomy; LAMS, lumen-apposing metal stent.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
