
Post written by Fatih Aslan, MD, from Advanced Endoscopy, Koc University Hospital, Istanbul, Turkey.

The procedure was performed with the patient under general anesthesia using a standard gastroscope. A submucosal tunneling approach was initiated proximal to the diverticulum. The surrounding tissue was carefully dissected, allowing the diverticulum to be mobilized into the lumen and subsequently inverted.
After repositioning the diverticulum into the lumen, we performed a selective myotomy using an intermuscular tunneling technique, followed by muscular-level suturing to reconstruct the functional outflow tract of the esophagus. The primary goal throughout the procedure was to restore luminal geometry in a way that supports physiological flow and facilitates passage of food into the stomach. In the final step, the diverticulum was resected, and the mucosal defect and tunnel entry were securely and safely closed.
In complex esophageal disorders such as epiphrenic diverticulum or advanced achalasia, outcomes may not be explained solely by the correct execution of technical steps. These conditions should be understood as manifestations of underlying pathophysiological processes shaped by the interplay of pressure balance, wall tension, and flow dynamics. Many of the clinical challenges we face today can be traced back to fundamental principles described by Blaise Pascal, Pierre-Simon Laplace, and early studies in flow physics.1,2
The purpose of sharing this video is to highlight the importance of approaching modern endoscopic therapy not only as a technical skill but also as a physiologically driven problem-solving process. Although technical success—defined as a safe, controlled, and adverse event—free procedure—remains a cornerstone of advanced endoscopy, it does not always translate into clinical or functional improvement.
With large epiphrenic diverticula, even after septotomy or septomyotomy, the diverticular reservoir may persist. This can lead to continued pressure imbalance within the esophagus, rendering food transit largely dependent on gravity. In the absence of peristalsis, myotomy alone may be insufficient to restore effective flow.
Because gravity cannot be modified, the physiological objective of treatment may be better defined as optimizing the pathway through which food reaches the stomach. In other words, reducing flow resistance and reshaping luminal geometry may, in select cases, provide more meaningful outcomes than conventional approaches.
For this reason, in the present case, we aimed to restore pressure-flow balance through reconstruction of the esophageal lumen. For us, this video represents not only a technical demonstration but also an example of the evolving paradigm in advanced endoscopy toward a more physiology-based approach.
One of the key takeaways is that technical success is not always synonymous with clinical success. Progress in advanced endoscopy appears to depend not only on technological advancements but also on the accurate interpretation of physiological principles and development of new treatment strategies accordingly. A clear paradigm shift is being observed from surgical approaches associated with organ loss or significant anatomical alteration toward function-preserving, minimally invasive endoscopic solutions. Furthermore, integration of suturing strategies into advanced endoscopic procedures may extend beyond defect closure and healing, potentially reshaping our therapeutic approach in complex conditions.
Advanced endoscopy continues to evolve rapidly. The introduction of techniques such as peroral endoscopic myotomy (POEM) and submucosal tunneling endoscopic resection has marked a major turning point in management of esophageal diseases, expanding the boundaries of minimally invasive therapy.
However, important questions remain unanswered. For example, in patients with markedly dilated or sigmoid esophagus, POEM can be technically successful, but clinical outcomes may not always be as satisfactory as in other types of achalasia. Over time, the POEM technique itself has evolved, shifting from longer anterior full-thickness myotomies toward shorter posterior approaches. These observations suggest that the answer may not lie solely in technical variations but rather in the combined evaluation of physiological principles and anatomical realities.
This case, along with our prior experience, was planned and performed within this framework—considering pressure balance, flow dynamics, and luminal geometry as interconnected factors. Ultimately, meaningful progress in advanced endoscopy may depend on the ability to integrate pathophysiology with anatomical understanding.
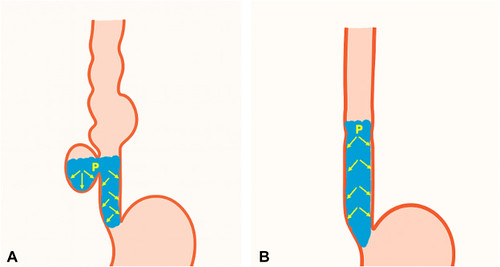
A, Pretreatment: accumulation of liquids and solid food increases intradiverticular and intraesophageal intraluminal pressure. B, Post-treatment: restoration of the tubular anatomy balances intraluminal pressure and increases flow velocity with gravitational force.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
