
Post written by Aman Deep, MD, from the Department of Nephrology, Asante Rogue Regional Medical Center, Medford, Oregon, USA.

Esophageal stents are used to relieve obstruction in diverse benign and malignant esophageal conditions.
However, excessive granulation tissue may make the removal of such stents challenging, and it increases the risk of adverse events such as bleeding and mucosal tear.
Various methods to remove embedded, partially covered self-expanding metal stents (PC-SEMSs)—such as the stent-in-stent technique, argon plasma coagulation (APC), piecemeal extraction, and retrieval using rat-tooth forceps—have been described in literature. Yet, the role of cryotherapy in retrieval of embedded stents has not been studied well so far.
This video case demonstrates the use of cryotherapy to remove an embedded, PC-SEMS after failure of the stent-in-stent technique, endo-loop cutter, and APC. Steris TruFreeze cryotherapy (Steris Healthcare, Dublin, Ireland) was applied to the proximal and distal ends of the embedded stent for 3 cycles of 20 seconds each. After frosting, each cryotherapy cycle consisted of spraying for 20 seconds before allowing 30 to 60 seconds for thawing.
At 3-week follow-up, the proximal end of the embedded stent appeared disimpacted. However, the therapy could not successfully disimpact the distal end from gastric mucosa.
This video demonstrates successful application of a known endoscopic technique (cryotherapy) in a new area of interest (removal of embedded esophageal stents).
Three cycles of cryotherapy for 20 seconds after frosting may be considered for embedded esophageal stent removal when other commonly used techniques are unsuccessful.
In conclusion, larger studies are needed to investigate the efficacy and safety of cryotherapy for this indication.
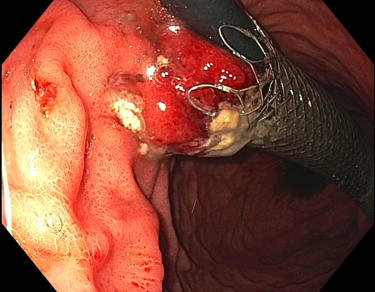 Distal end of stent was seen embedded in a granulomatous mass in gastric mucosa.
Distal end of stent was seen embedded in a granulomatous mass in gastric mucosa.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
