
Post written by Michael Fernandez Y Viesca, MD, from the Department of Gastroenterology Hepatopancreatology and Digestive Oncology, Erasme Hospital, Brussels, Belgium.

This video case shows how challenging it can be to choose the correct insertion route (anterograde vs retrograde) before an enteroscopy based on video-capsule time index landmarks.
Indeed, these time indexes are not always reliable for identifying the precise localization of a lesion, as shown in this video case.
In some cases, other imaging techniques help us choose the correct approach, or the alternative route will be necessary to reach a lesion.
It is important for us to show how to deal with and overcome these issues in daily practice. Careful video-capsule overview and reporting as well as consideration of all available clinical information (including other imaging) are crucial.
This also highlights the importance of caution when using the motorized spiral enteroscope, a safe and effective device-assisted enteroscopy that, however, requires expertise and optimal patient selection.
Taking care of patients requiring small-bowel exploration goes beyond reading the video-capsule and performing enteroscopy. A patient-centered approach should be adopted. This includes reviewing all available clinical information, choosing the optimal device and route, and adapting management according to the findings.
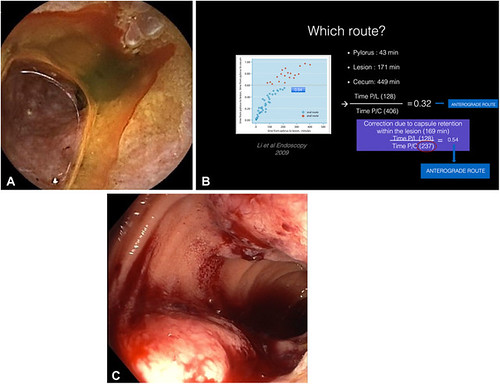
A, Actively bleeding obstructive lesion visualized through the video-capsule endoscopy in the ileum. B, The lesion’s time-index location is calculated as the ratio of the transit time from the pylorus to the lesion and the transit time from the pylorus to the cecum, suggesting an anterograde approach. (Adapted from: Li X, Chen H, Dai J, et al. Predictive role of capsule endoscopy on the insertion route of double-balloon enteroscopy. Endoscopy 2009;41:762-6.) C, Hemi-circumferential lesion localized 70 cm above the ileocecal valve identified during the retrograde motorized spiral enteroscopy.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
