
Post written by Stefano Crippa, MD, PhD, from the Division of Pancreatic Surgery, IRCCS San Raffaele Scientific Institute, and Vita Salute San Raffaele University, Milan, Italy, Fabio Giannone, MD, from the Division of Pancreatic Surgery, IRCCS San Raffaele Scientific Institute, and the Department of General, Digestive and Endocrine Surgery, University Hospital of Strasbourg, Strasbourg, France, and Massimo Falconi, MD, from the Division of Pancreatic Surgery, IRCCS San Raffaele Scientific Institute and Vita Salute San Raffaele University.

The management of pancreatic cystic neoplasms (PCNs) is complex when considering the difficulties in differential diagnosis and the appropriate surgical indications (ie, symptoms and/or malignancy-related features). Proper preoperative diagnosis can be inaccurate in nearly 20% to 30% of patients, and cross-sectional imaging is considered the “first-level” diagnostic tool for characterizing PCNs.
The role of EUS is less defined in clinical practice because of numerous inconsistencies in guidelines and the limited availability of a high-level procedure.

We reviewed all diagnostic workup of pancreatic resections for PCNs over 10 years. In a high-volume tertiary center for pancreatic surgery, almost 600 PCNs were resected, and two-thirds of these underwent EUS preoperatively. We compared the value of this procedure, performed by experienced endosonographers, with standard radiology in terms of improving the diagnostic yield over the years.
Diagnostic accuracy for PCNs is still far from optimal, and about 20% of preoperative diagnosis did not match with final histology, even in a tertiary center. The rate of correct diagnosis in patients who underwent EUS is significantly higher than those who underwent radiology-only workup.

Among all the criteria assessed, main pancreatic duct dilatation and cytology obtained through FNA are the only variables independently associated with the accuracy of the presumed diagnosis. Risk of incorrect diagnosis is correlated with that of performing an unnecessary surgery, which is a benign pathological report that did not show risk of malignancy and immediate absolute indication.
Younger age, a cyst >3 cm, and undergoing a distal pancreatectomy rather than a pancreatoduodenectomy are the other features found to be correlated with the risk of inappropriate resection.
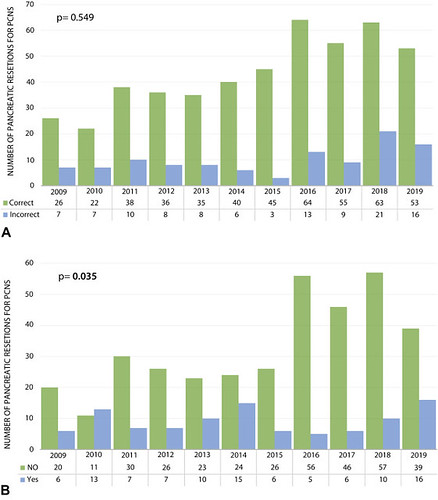
A, Rate of diagnostic accuracy over the 10-year period. B, Rate of delayable surgery over the 10-year period. PCNS, Pancreatic cystic neoplasms.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
