
Post written by Hiromu Fukuda, MD, from the Department of Gastroenterology and Hepatology, Osaka University Graduate School of Medicine, Suita, Japan.

In this video case, we show the usefulness of endoscopic submucosal dissection (ESD) in the right lateral position (RLP) for early gastric cancer (EGC) in the fornix. ESD of EGC in the fornix is challenging because the lesion is difficult to approach and tends to face vertically in the left lateral position (LLP).
In addition, the lesion is occasionally immersed in gastric fluid and blood, interfering with the procedure because of poor visibility. Despite the use of a multibending scope or previously attempted clip traction techniques, some technical difficulties remain. The RLP can counter the gravity and change the approach to the fornix. We present the case of a fornix ESD performed in the RLP.
A man in his 80s with a history of pyloric gastrectomy underwent surveillance EGD that revealed the presence of a metachronous EGC in the fornix. Because the patient had a high risk of difficulty with airway management after radiotherapy for pharyngeal cancer, he underwent ESD under general anesthesia.
The procedure was performed using a single-channel endoscope (GIF-Q260J; Olympus Co, Tokyo, Japan) with an ITknife2 (Olympus Co) and a FlushKnife BTS (Fujifilm Co, Tokyo, Japan). First, at the LLP, part of the lesion was submerged in water, and an optimal intraoperative view could not be obtained. Therefore, we moved the patient to the RLP. The reversed gravity spared the lesion from submersion.
Furthermore, tangential proximity to the submucosal space and favorable countertraction by gravity were attained until complete resection was achieved. The patient started oral intake 2 days after ESD and was discharged without complications. Histopathological examination confirmed a curative resection.
We demonstrate that the RLP facilitated fornix ESD under general anesthesia by avoiding submersion, enhancing accessibility, and allowing beneficial countertraction without the need for specialized equipment.
In conclusion, ESD for EGC has become common as a standard treatment. However, some technical difficulties remain. ESD for EGC in the fornix is challenging, and the lesion is occasionally immersed, resulting in interference with the procedure. Although useful devices such as a traction device and a multibending scope are available, switching the position from the LLP to the RLP is considered simpler and more effective.
Because ESD in the RLP is very simple and effective, endoscopists can take advantage of this method in daily clinical practice.
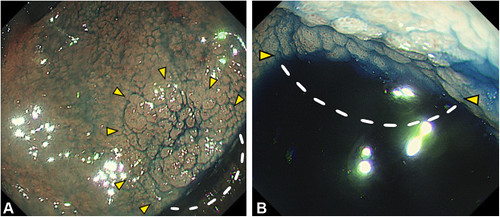 Endoscopic views (A, retroflex view; B, forward view) in the left lateral position showing the pull of gravity toward the fornix side and that a part of the lesion is submerged in water. Yellow arrowheads indicate the demarcation line of the lesion. Dotted lines indicate the lesion area submerged in water.
Endoscopic views (A, retroflex view; B, forward view) in the left lateral position showing the pull of gravity toward the fornix side and that a part of the lesion is submerged in water. Yellow arrowheads indicate the demarcation line of the lesion. Dotted lines indicate the lesion area submerged in water.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
