
Post written by Eric E. Low, MD, MPH, and Rena Yadlapati, MD, MSHS, from the Division of Gastroenterology, University of California San Diego, San Diego, California, USA.

Achalasia is the most well-characterized esophageal motility disorder largely because of evolving diagnostic tools and physiologic research that have been developed over the last 2 decades.

With the Chicago classification now in its fourth iteration, 3 distinct subtypes of achalasia have been characterized using esophageal high-resolution manometry. The identification of achalasia subtypes has led to improved clinical outcomes, as treatment recommendations vary among subtypes.
Currently, surgical Heller myotomy, pneumatic dilation, and peroral endoscopic myotomy (POEM) are first-line therapies for type 1 and type 2 achalasia. However, POEM is the first-line therapy recommended for type 3 achalasia.
Since the inception of POEM by Dr. Haruhiro Inoue and his team in 2009, the technique has remained relatively unchanged. Adaptations to myotomy thickness and length have been studied to improve clinical outcomes, reduce rates of post-POEM GERD, and limit overall procedure time. We describe the evolution of these adaptions in our review of POEM for achalasia.
Incidence and prevalence of achalasia have been increasing. Now that POEM has become standard practice at many GI centers throughout the United States, we wanted to summarize the evidence regarding the POEM technique to promote best practices based on the current literature.
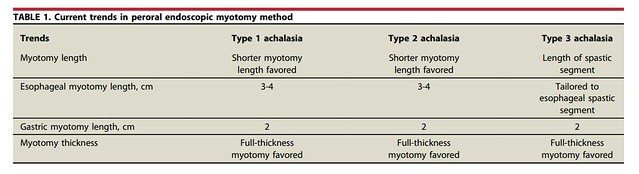
The POEM technique has evolved since its inception in 2009. Based on current literature, it is recommended to perform a full-thickness myotomy regardless of subtype. A short esophageal myotomy (3-4 cm) with a 2-cm extension into the gastric side is the recommended length of myotomy for type 1 and type 2 achalasia, whereas a tailored esophageal myotomy (based on spastic segment) with a 2-cm extension into the gastric side is recommended for type 3 achalasia.
As the procedure technique becomes more widely practiced, efforts should focus on promoting multidisciplinary and individualized patient care for those with achalasia. For instance, patients with type 3 achalasia should be offered POEM with an extended proximal myotomy, as is reflected in societal guidelines from the American Society for Gastrointestinal Endoscopy and the American College of Gastroenterology.
In addition, all patients should be counseled on their individual risks for adverse events, including postprocedural GERD, as well as such considerations as time off work, length of hospital stay, and potential for reintervention.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
