
Post written by Shi Wang, MD, from the Department of Endoscopy, The Cancer Hospital of the University of Chinese Academy of Sciences (Zhejiang Cancer Hospital), Institute of Basic Medicine and Cancer (IBMC), Chinese Academy of Sciences, Hangzhou, China.

The quality of EGD is a prerequisite for a high detection rate of upper GI lesions, especially early gastric cancer. Our previous study showed that an artificial intelligence (AI) system (named intelligent detection endoscopic assistant [IDEA]) could help monitor blind spots and provide an operation score during EGD.
We verified the effectiveness of IDEA to help evaluate the quality of EGD in a large-scale multicenter trial.
In the past few years, AI technology has made remarkable progress in the field of endoscopy. Most studies are dedicated to the use of computer-aided diagnosis of lesions. However, to the best of our knowledge, there has been no study on the use of AI for quality control in a large-scale multicenter trial to inspect upper GI cancer.
In the present study, IDEA–a real-time quality control system based on the deep convolutional neural network and long short-term memory for monitoring blind spots, timing the procedure, and generating photo documentation during EGD–was developed. IDEA can give a score based on blind spots and photo quality during EGD. We equipped IDEA in 12 hospitals and found that the cancer detection rate and the early cancer detection rate were positively correlated with a score given by IDEA.
As a study that applies AI to evaluate EGD quality on a large scale, this research has given us some preliminary hints that standardized EGD is very important for the detection of upper GI cancer. AI technology provides an objective evaluation method, and the score of AI shows a correlation with the detection rate. The role of AI in screening early digestive tract cancer needs to be confirmed by additional large-scale clinical trials.
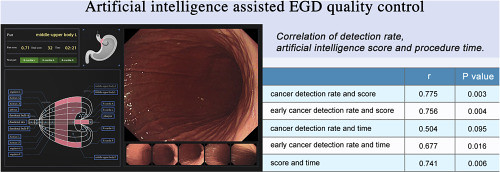
Graphical Abstract
The left shows a working example of IDEA. The regression lines and Pearson correlation suggest that the cancer detection rate in each hospital was positively correlated with total score (r = .775, P = .003). Similarly, the early cancer detection rate was positively correlated with total score (r = .756, P = .004). The early cancer detection rate in each hospital was positively correlated with the average endoscopic procedure time (r = .677, P = .016).
However, there was no significant correlation between the cancer detection rate and the operation time (r = .504, P = .095). The total score was correlated with the average procedure time (r = .741, P = .006).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
