
Post written by Kazunari Nakahara, MD, PhD, from the Department of Gastroenterology and Hepatology, St. Marianna University, School of Medicine, Kawasaki, Japan.

We present a case of successful endoscopic transpapillary gallbladder stenting (EGBS) via straightening of the guidewire that looped in the neck of the gallbladder using a stone retrieval balloon catheter.
A 76-year-old woman with right upper quadrant pain and high fever was admitted to our hospital and diagnosed with segmental adenomyomatosis (ADM) and acute cholecystitis on the fundus segment of the gallbladder. Considering the high surgical risk owing to poor physical condition, we performed EGBS.
After bile duct cannulation, a hydrophilic guidewire could be advanced into the fundus of the gallbladder, and it was changed to a 0.025-inch stiff type. However, the guidewire was large looped in the neck of the gallbladder because of segmental ADM that could not be straightened by the guidewire and cannula manipulation, and the plastic stent could not be placed into the fundus of the gallbladder.
Thus, a balloon catheter for stone retrieval with a balloon diameter of 18 mm (Extraction Balloon Catheter; Zeon Medical Inc, Tokyo, Japan) was inserted into the fundus of the gallbladder, and the balloon was inflated.
Then the catheter was pulled by anchoring the balloon on the narrow part of the ADM, thereby successfully straightening the catheter and the guidewire. After straightening the guidewire, a 5F, 10-cm pigtail plastic stent was successfully placed into the fundus of the gallbladder without difficulty.
EGBS is technically challenging. In some patients, a stent cannot be placed into the fundus of the gallbladder because of the looped guidewire in the cystic duct or the neck of the gallbladder. The technique of straightening the guidewire using a stone retrieval balloon catheter can be a useful option in EGBS.
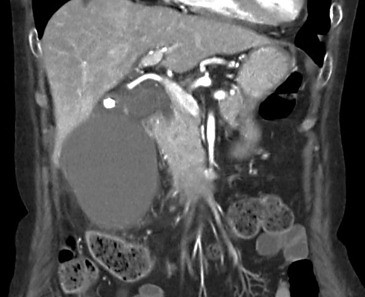 CT showed segmental adenomyomatosis and acute cholecystitis on the fundus segment of the gallbladder.
CT showed segmental adenomyomatosis and acute cholecystitis on the fundus segment of the gallbladder.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
