
Post written by Donevan Westerveld, MD, from the Division of Gastroenterology & Hepatology, NewYork-Presbyterian Hospital/Weill Cornell Medicine, New York, New York, USA.

A high-grade malignant small-bowel obstruction (SBO) is typically managed with surgical diversion (ileostomy) or palliative decompression via nasogastric tube or venting gastrostomy. These approaches have a significant impact on a patient’s quality of life.
We describe the case of a 91-year-old man with a high-grade SBO at the ileocolonic anastomosis (prior hemicolectomy due to colon cancer) who deferred surgical diversion with ileostomy in favor of endoscopic bypass via EUS-guided ileosigmoidostomy.
Management of high-grade malignant SBOs in a patient deemed a nonoperative candidate has traditionally been limited to placement of a venting percutaneous endoscopic gastrostomy.
However, this approach is often in stark contrast to the patient’s and family’s wishes to be able to eat near the end of his or her life. With the advent of the lumen-apposing metal stent (LAMS) and improved endoscopic techniques, we can now offer patients alternative and minimally invasive methods at decompression of a high-grade SBO.
Successful endoscopic decompression of malignant SBOs by creating an enterocolostomy into the proximal colon have been reported in the literature. However, the aforementioned approaches were technically challenging and time-consuming, as they required advancing an echoendoscope to the proximal colon, which is not always possible.
In this video, we demonstrate that decompression of the small bowel into the distal colon using a LAMS via ileosigmoidostomy can successfully palliate SBO, obviating the need for a challenging proximal colon procedure. Our method decreased overall procedure time, eliminated the need for a forward-viewing echoendoscope, and relieved the obstruction, allowing the patient to continue comfort feeding without development of post-procedure diarrhea.
It is important to note that we accounted for the prospect of diarrhea by ensuring that we performed the bypass with at least 20-30 cm of distal colon remaining.
The options for endoscopic management of nonoperative malignant SBOs have grown to encompass decompression via EUS-guided LAMS by creating an enterocolostomy. Creation of an EUS-guided ileosigmoidostomy is effective at decompressing the small bowel, allows the patient to continue oral intake, and does not significantly impact a patient’s quality of life in terms of post-procedure-related diarrhea, as long as sufficient sigmoid colon remains.
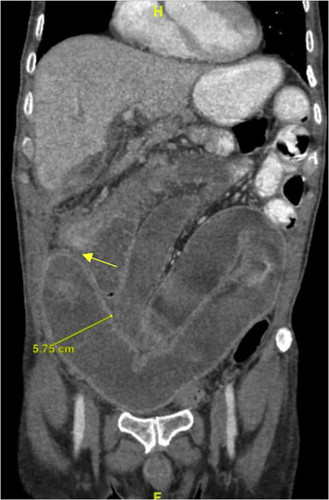
CT scan showing a high-grade small-bowel obstruction (yellow arrow) and dilation.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
