
Post written by Jeska A. Fritzsche, MD, from the Department of Gastroenterology and Hepatology, Amsterdam University Medical Center, Amsterdam Gastroenterology Endocrinology & Metabolism, Amsterdam, the Netherlands.
The focus of our study was to assess the expected wide variety in daily practice of endoscopic papillectomy and to achieve further consensus among international experts by using a Delphi process.
Endoscopic papillectomy is considered the preferred treatment method to resect papillary adenomas in patients without invasive disease. Although considered a safe and viable alternative to surgery, the endoscopic resection of papillary adenomas is still accompanied by a considerable risk of adverse events and recurrence. In order to mitigate the risk of these events, it is essential to further refine the procedure. However, due to the low incidence, it is difficult to perform large prospective and randomized controlled studies, leading to a paucity of high level scientific knowledge and subsequent current absence of evidence-based guidelines.
We sought to address this deficiency by using a Delphi process, which led to the first consensus-based management algorithm for papillary adenomas. This study can therefore be considered a first vital step in aligning the execution of the procedure in daily practice and shows important aspects of the procedure on which future studies should focus, aiming to be able to substantiate a more robust evidence-based consensus guideline in the future.
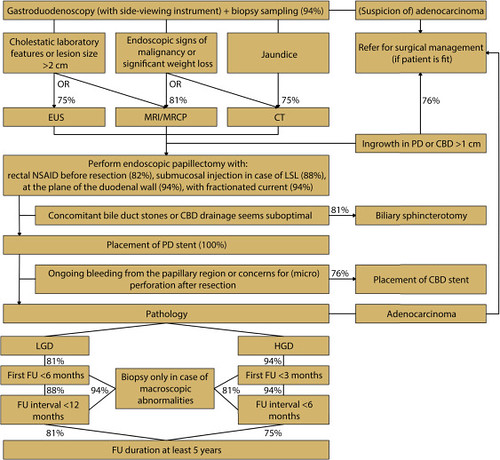
Figure 2. Consensus-based flowchart. Percentages indicate degree of agreement. CBD, Common bile duct; CT, computed tomography; EUS, endoscopic ultrasound; FU, follow-up; HGD, high-grade dysplasia; LGD, low-grade dysplasia; LSL, laterally spreading lesion; MRCP, magnetic resonance cholangiopancreatography; MRI, magnetic resonance imaging, NSAID, nonsteroidal anti-inflammatory drug; PD, pancreatic duct.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
