
Post written by Saurabh Chandan, MD, from the Gastroenterology and Hepatology, CHI Creighton University Medical Center, Omaha, Nebraska, USA.

Underwater endoscopic mucosal resection (U-EMR) is a simple and easy-to-learn technique for resection of colorectal lesions. It eliminates the need of using submucosal injection to “lift” the lesion prior to resection. The main aim of our study is to compare outcomes of U-EMR and conventional endoscopic mucosal resection (C-EMR) in colorectal polyps with special focus on large (>20 mm) lesions.
An important factor in interval development of colorectal cancer (CRC) is the incomplete resection rate of polyps during colonoscopy. This rate is significantly higher for sessile serrated lesions particularly those between 10 mm and 20 mm in size. Lesions larger than 20 mm in size have an even greater risk of incomplete resection. While the safety and efficacy of U-EMR has been previously reported, it’s outcomes in comparison to C-EMR have only been reported in a few cohort and randomized controlled studies. We performed a systematic review and meta-analysis of the efficacy and safety outcomes of the 2 techniques based on current body of evidence.
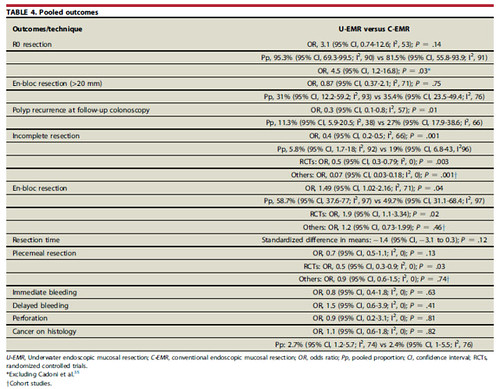
Our analysis included 1851 patients from 11 studies, including 4 randomized controlled trials (RCTs). A total of 1071 lesions, 295 of which were >20 mm in size, were removed using U-EMR and 1049 lesions, 296 of which were >20 mm in size, were removed using C-EMR. We found that while U-EMR has a higher success rate of en bloc resection as compared to C-EMR, rate of R0 resection, defined as complete resection of a lesion with tumor-free lateral and vertical margins, is comparable between the 2 techniques. U-EMR also had lower rates of polyp recurrence and incomplete resection.
When comparing outcomes strictly from RCTs, we found that U-EMR performs significantly better than C-EMR with regards to successful en bloc and piecemeal resection at index colonoscopy. We found no statistically significant difference between the 2 techniques when comparing resection times and en bloc resection of colorectal lesions larger than 20 mm. Both techniques also have a similar safety profile in terms of immediate and delayed bleeding, as well as perforation. Finally, there was no statistically significant difference in the accuracy of the 2 techniques for diagnosing CRC on histology from resected specimens.
As more randomized controlled trials are carried out comparing these 2 techniques, we feel there will be more robust evidence to support the routine use U-EMR for colorectal polyps. We also eagerly await more long-term follow-up data to evaluate adenoma recurrence with both techniques.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
