
Post written by Hideaki Harada, MD, from the Department of Gastroenterology, New Tokyo Hospital, Chiba, Japan.

Our study aimed to clarify the risk of postpolypectomy bleeding (PPB) after endoscopic snare resection of colorectal polyps in patients receiving continuous warfarin and 1-day cessation of direct oral anticoagulants (O-DOACs) because the evidence for use of continuous anticoagulants for endoscopic snare resection of colorectal polyps was insufficient in patients receiving warfarin or DOACs.
Conventional managements of anticoagulants in patients with colonic polypectomy, like stopping anticoagulants or replacing anticoagulants by heparin bridge therapy, are associated with high rates of delayed bleeding and thromboembolic events.
Although patients with continuous use of warfarin and 1-day cessation of DOACs had high rates of PPB in comparison with those without use of these anticoagulants, O-edoxaban showed a lower rate of PPB compared with other DOACs including O-rivaroxaban (O-edoxaban, 1.8%; O-dabigatran, 6.1%; O-rivaroxaban, 14.8%; and O-apixaban, 9.8%). Edoxaban may be safe through short-term withdrawal for endoscopic snare resection of colorectal polyps; this should be confirmed by a future prospective study.
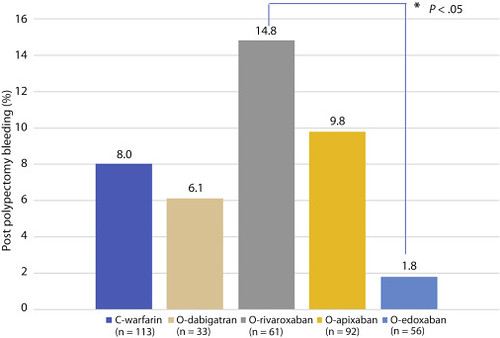
Figure 1. Postpolypectomy bleeding (PPB) rate with continuous warfarin (C-warfarin) and 1-day cessation of direct oral anticoagulants (O-DOACs). PPB was observed in 9 patients in the C-warfarin group and in 21 patients in the O-DOACs group: C-warfarin (8.0% [9/113]), 1-day cessation of (O-) dabigatran (6.1% [2/33]), O-rivaroxaban (14.8% [9/61]), O-apixaban (9.8% [9/92]), and O-edoxaban (1.8% [1/56]). The PPB rate in the O-rivaroxaban group was significantly higher than that in the O-edoxaban group (P < .05).
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
