
Post written by Andrea Lisotti, MD, from the Gastroenterology Unit, Hospital of Imola, Department of Medical and Surgical Sciences, University of Bologna, Bologna, Italy. 
Endoscopic ultrasound (EUS) has a pivotal role in the management of pancreatic cancer, one of the most lethal neoplasms with a 5-year survival that has not significantly increased over the last decades. In this setting, EUS was demonstrated to be accurate for the detection even of small lesions, for local staging, and for tissue sampling. EUS-guided tissue sampling is indicated in all patients with borderline-resectable, unresectable, or metastatic PC, although its role in resectable masses is still debated but nevertheless often required, based on local multidisciplinary team consensus.
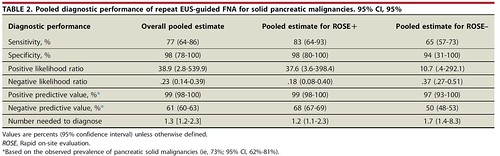
Despite all the recent technical improvements, a non-negligible risk of false-negative or inconclusive results with EUS-guided tissue sampling still exists. In such cases, major guidelines recommend repeating EUS-guided tissue sampling. The value of repeat EUS-FNA (rEUS-FNA) after an initial negative examination was investigated by different studies, reporting sensitivity for the diagnosis of malignancy in the range of 35% to 100%. The focus of our study was to evaluate the pooled diagnostic sensitivity and specificity of rEUS-FNA for the diagnosis of solid pancreatic masses after a previous non-diagnostic or inconclusive EUS-FNA.
The results of this study objectively substantiated the added value of rEUS-FNA for the diagnosis of solid pancreatic masses in cases of a previous non-diagnostic or inconclusive result. To date, the management of patients with suspected pancreatic cancer and a previous negative EUS-FNA results was not based on high-quality evidence. Several guidelines recommend repeat biopsy sampling, while clinical follow-up was proposed in low-risk cases. Overall, although not evidence-based, it is common practice to perform rEUS-FNA worldwide.
We believe that our results provide high-quality evidence supporting the practice of rEUS-FNA after initial non-diagnostic or inconclusive tissue sampling. The optimal pooled specificity coupled with the low false-positive rate demonstrate that a rEUS-FNA substantially increases the diagnostic yield. Based on our data, we observed that this strategy may change the diagnostic and therapeutic approach in up to 60% of cases (80% if rapid on-site evaluation, ROSE, was available).
Briefly, our results corroborate the current practice and guidelines, demonstrating that in case of a rEUS-FNA positive for malignancy the result is highly reliable, whereas a negative result significantly reduces the risk of underlying malignancy.
The sub-group analysis conducted according to the presence of ROSE suggested an interesting topic; in detail, studies conducted with ROSE showed a higher sensitivity with a slightly higher specificity as compared with studies without ROSE. Furthermore, a correct rEUS-FNA diagnosis was achieved in 8 of 10 patients with ROSE versus 6 of 10 patients without ROSE. Because the role of ROSE, after initial enthusiasm, is undergoing a downsizing of its applications, our findings are relevant because they strongly support the implementation of ROSE for the particular setting of rEUS-FNA. In this context, ROSE may bring a significant increase in definitive diagnosis, thereby reducing the need for further examinations and healthcare-related costs.
Among several technologic, technical, and knowledge innovations, the introduction of EUS-FNB needles into clinical practice have significantly influenced daily EUS-guided tissue acquisition methods and results. To date, no data on the role of EUS-FNB sampling after nondiagnostic or inconclusive (rEUS-FNB) results are available, we can only hypothesize that these results could be replicated in this setting. We think that future research should focus on the evaluation of the diagnostic performance of rEUS-FNB even in comparison to rEUS-FNA to confirm our findings and move forward further implementations.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
