
Post written by Mayenaaz Sidhu, MBBS, from the Department of Gastroenterology and Hepatology, Westmead Hospital, and Westmead Clinical School, The University of Sydney, Sydney, New South Wales, Australia.
The focus of this study was to assess long-term outcomes of sized-matched laterally spreading colorectal lesions (LSL) resected en bloc (e-EMR) as compared to piece-meal resection (p-EMR).
e-EMR has been preferred over p-EMR primarily due to the reported reduced recurrence rates at surveillance. However, e-EMR is limited by lesion size, with lesions >25 mm associated with an increased rate of muscularis propria injury. Thus, size is a major confounder when comparing these 2techniques, and to date no large prospective trials have compared lesions of similar size when resected by e-EMR versus p-EMR. We therefore designed this trial to assess the short- and long-term outcomes with regard to safety and efficacy of both techniques for lesions of similar size.
In this large prospective trial of 570 LSL, of which 45.4% were resected by e-EMR, p-EMR was equally efficacious for the treatment of colonic LSL ≤25 mm. In fact, e-EMR was associated with an increased risk of major deep mural injury when compared to p-EMR (3.5% vs 1.0%, P=0.05). Thus, LSL ≤ 25 mm can be safely removed p-EMR with e-EMR or alternate en bloc resection techniques reserved for lesions suspicious for invasive disease.
It should be noted the data in this study predates the use of thermal ablation of the post-EMR defect margin, which if routinely implemented is likely to further reduce the risk of recurrence and the perceived benefit of e-EMR of 20-25 mm LSL. This should be evaluated further in large multi-center prospective trials.
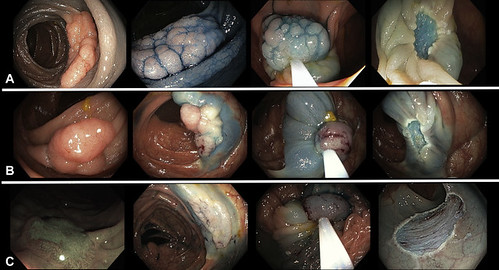
Figure 1. Examples of e-EMR. A, 20 mm, Kudo III, granular laterally spreading lesions (LSLs) in the sigmoid colon. B, 25 mm, Kudo III, granular LSLs in the ascending colon. C, 20 mm, Kudo V, nongranular LSLs in the ascending colon.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
