
Post written by In Kyung Yoo, MD, PhD, from the Department of Gastroenterology, Cha Bundang Medical Center, Cha University College of Medicine, Seongnam-si, Korea.

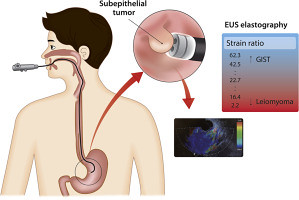
EUS elastography is a real-time imaging technique that displays the tissue elasticity differences between diseased and normal tissues on the conventional B-mode ultrasound images. It analyzes the degree of tissue deformation under compression and reflects this information as a hue color spectrum. Most studies on quantitative EUS elastography investigate it in the context of pancreatic diseases and propose a cut-off strain value for malignant lesions. We aimed to investigate the feasibility of EUS elastography in the differential diagnosis of the gastric SETs based on strain ratio.
As a minimally invasive method, EUS elastography plays an important role in assessing malignancies of the GI tract and nearby organs. Elastography adds valuable information to EUS elastography by providing a quantitative evaluation of tissue stiffness, thus reflecting the malignant or benign nature of the disease. This is a first study that presents cut off value for differentiating GIST for other gastric SETs and emphasizes the role of EUS elastography in gastric SETs.
Our results demonstrated that lipomas and leiomyomas had lower strain ratios, whereas GISTs and schwannomas showed relatively higher strain ratios. Based on our results, if the lesion is suspicious for either leiomyoma or GIST on EUS interpretation, a strain ratio >22.7 favors GIST rather than leiomyoma with sensitivity of 100% and specificity of 94.1%. This suggests that additional elastography might enhance the diagnostic accuracy of EUS for the differential diagnosis of gastric SETs.
Further studies should include more various risk groups of GISTs and evaluate the elastic difference among them; this invasive screening test would be more useful. We would also evaluate strain ratio based on tumor size and location in our next study.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
