
Post written by Madhav Desai, MD, MPH, from the Gastroenterology and Hepatology, University of Kansas Medical Center, Kansas City, Kansas, USA.

Colonoscopy prevents colon cancer and, therefore, has become a widely used screening modality. Right-sided lesions are often missed during standard colonoscopy and could account for interval colon cancer. As gastroenterologists and endoscopists, our keen focus has been to improve adenoma detection rates (ADR) in the right colon. Due to anatomy, type of lesions (sessile and flat lesions are more common), and prep factors, subtle lesions could be missed.
A second forward-view examination or retroflexion in the right side of the colon have been proposed as techniques to improve ADR in the right side of the colon. Comparative data on examining the right side of the colon with a second forward view or retroflexion is not known in a pooled analysis.
Missed lesions on the right side of the colon could contribute to interval colon cancers, and research has shown that there has been an increase in post-colonoscopy interval colorectal cancer. It is critically important that we spend adequate time in the right colon on withdrawal and do a thorough cleaning to find any subtle lesions to improve the quality of a screening colonoscopy. However, at the same time, despite our best efforts, lesions can be missed as they can hide behind thick folds in the ascending colon and near the hepatic flexure. Repeat look with retoflexion has shown to improve detection of such lesions, but retroflexion can be technically challenging and raise the risk of perforation. Second forward-view exam, on the other hand, has been shown to improve the yield as well. We performed a systematic review of the literature to assess the yield of a second forward view compared with retroflexion examination for the detection of right-sided adenomas.
In this systematic review, we showed that a double right colon exam is important and increased overall gain compared to a single exam, irrespectively if done by second forward view or retroflexion. The pooled adenoma miss rate of single forward exam was 13.3% (95% CI, 6.6%-20%) when compared to second forward view and 8.1% (3.7%-12.5%) when compared to retroflexion. No statistically significant difference was noted when second forward view and retroflexion were compared in terms of adenoma miss rate (7.3% vs 6.3%; pooled odds ratio, 1.2; 95% CI, 0.9-1.61; P = .21). Second forward view of the right side of the colon increased the right-sided ADR by 10% (n = 4; second forward view vs SC, 33.6% vs 26.7%) with a pooled risk difference of 0.09 (95% CI, 0.03-0.15; P < .01). Retroflexion increased the right-sided ADR by 6% (n = 3; retroflexion vs SC, 28.4% vs 22.7%) with a pooled risk difference of 0.06 (95% CI, 0.03-0.09; P < 01).
In short, meticulous right colon exam with a repeat look is essential and could be done by second forward view or retroflexion. After standard withdrawal, a second forward view and retroflexed view of the right side of the colon are both associated with improvement in ADR. One of these techniques should be considered during standard colonoscopy to increase ADR and to improve the quality of colonoscopy.
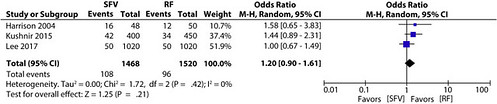
Figure 2. Adenoma miss rate of second forward view compared with retroflexion examination after a standard colonoscopy. CI, Confidence interval; M-H, Mantel-Haenszel; SFV, second forward view; RF, retroflexion.
Read the full article online.
The information presented in Endoscopedia reflects the opinions of the authors and does not represent the position of the American Society for Gastrointestinal Endoscopy (ASGE). ASGE expressly disclaims any warranties or guarantees, expressed or implied, and is not liable for damages of any kind in connection with the material, information, or procedures set forth.
